
Join over 1,000 people in helping the Paula Takacs Foundation raise crucial funds for groundbreaking research and clinical trials, all while spreading awareness to accelerate diagnoses and save lives.
Announcing the $2 Million Paula Takacs Foundation Endowed Chair of Sarcoma Research

The Paula Takacs Foundation for Sarcoma Research is immensely proud to announce the establishment of the Paula Takacs Foundation Endowed Chair of Sarcoma Research at Levine Cancer Institute, supported by a $2 Million endowment fund.
We know Paula would be so proud, and maybe not even surprised, because it was her relentless commitment to her vision to change the outcome for sarcoma patients in Charlotte and around the world that catalyzed this historic announcement.
Take a few moments to watch Susan Udelson announce the endowment, and then read our Q&A to fully understand all facets of this monumental gift and its local and global impact on sarcoma research.
Q: What is an Endowed Chair?
A: An Endowed Chair is one of the highest honors in academic medicine. These positions are often reserved for full professors who are perceived as being the best of the best in their area of expertise. There are few Endowed Chairs of Sarcoma Research in the U.S., and who receive this type and level of funding for sarcoma research.
Q: Why create this Endowed Chair position?
A: At the heart of every great cancer center are scholars whose work is supported by endowed funds. Endowed Chairs create opportunities for these institutions to attract and retain distinguished professors who will significantly drive and impact a particular area of study and elevate the reputation of the organization itself. Endowed positions recognize outstanding faculty, acknowledge their professional standing and provide substantial support for the conduct of scholarly work and research.
Q: Who is appointed as Endowed Chair?
A: A professor level faculty who is an expert in sarcoma research will receive this prestigious appointment by the President of Levine Cancer Institute and other Atrium Health leadership during a forthcoming announcement and investiture ceremony. Stay tuned to find out who Levine Cancer Institute names as the inaugural Paula Takacs Foundation Endowed Chair!
Q: What are some benefits of establishing the Endowed Chair at Levine Cancer Institute?
A: There are many! The Paula Takacs Foundation Endowed Chair will direct the use of this $2 million endowment. It is the Chair’s responsibility to use a portion of these special funds at their discretion, each and every year, to advance science in the most strategic and novel ways possible. The endowment will ensure Levine Cancer Institute’s dedicated focus on this disease for all eternity! For Paula’s family, it keeps her name and beautiful legacy growing stronger forever too! It also brings national exposure and recognition to the Levine Cancer Institute sarcoma research program and Paula Takacs Foundation, attracting additional sarcoma talent to our region and ultimately benefiting patients throughout the globe.
Q: What is an Endowment Fund?
A: An endowment fund exists in perpetuity and is part of the long-term capital base of the cancer center. Earnings from the endowment are an ongoing source of support, despite fluctuations in the economy. A strong endowment allows the cancer center to plan for the future while continuing to drive innovation and research.
Q: What is the difference between this new $2 million Endowment and the longstanding Paula Takacs Sarcoma Research Fund?
A: The $2 million Endowment has been funded to solely support research at Levine Cancer Institute, as envisioned by the Paula Takacs Foundation Endowed Chair and reviewed by the Endowment Committee. The Paula Takacs Sarcoma Research Fund continues to operate separately, supporting cutting-edge studies and clinical trials at Levine Cancer Institute and/or Levine Children’s Hospital at the direction of Fund’s Advisory Committee.
Want to keep up to date with all the latest sarcoma news, educational materials, foundation developments, and cancer resources? Sign up for our monthly newsletter.
Want to get involved in the work of our foundation? Here are some ways you can make a huge difference.
Trial Results Confirm Effectiveness of Atezolizumab Against a Rare Sarcoma
Trial Results Confirm Effectiveness of Atezolizumab
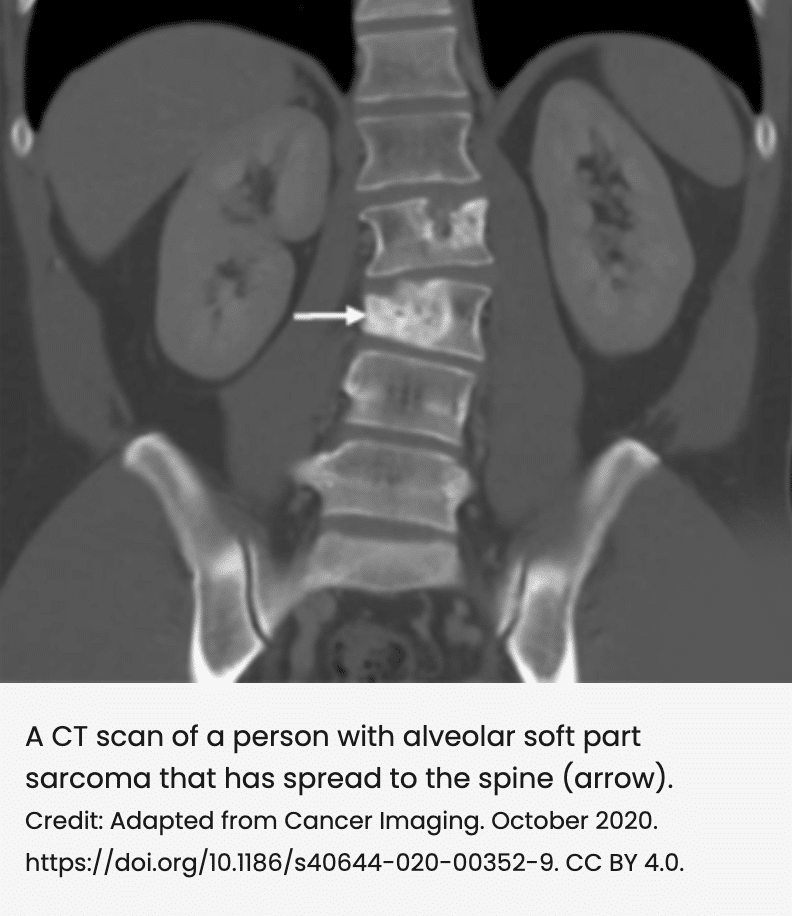
Faithanne Hill was only 11 when she was diagnosed with alveolar soft part sarcoma, an extremely rare soft tissue cancer that is diagnosed in only about 80 people (mostly adolescents and young adults) in the United States each year. Now 21, the first-year college student has been through a lot over the past decade.
In addition to going through the usual teenage experiences in her home country of Trinidad, she’s also had a half dozen or so surgeries at the NIH Clinical Center in Bethesda, MD, to remove new tumors that seemed to develop out of nowhere—a common occurrence for this cancer.
So far, the surgeries have kept her disease at bay. But Faithanne said she worries that, one day, surgery won’t work anymore, and she will have few treatment options. Chemotherapy generally doesn’t work for alveolar soft part sarcoma.
Several years ago, Faithanne joined a clinical trial to see whether the immunotherapy drug atezolizumab (Tecentriq) could help shrink her tumors. Results of that study, which included 52 people with advanced alveolar soft part sarcoma, were published September 7 in the New England Journal of Medicine.
All 52 people in the trial were treated with atezolizumab. Of these, 19 (37%) saw their tumors shrink by at least 30% (partial response), and one person’s tumors disappeared altogether (complete response). Patients who were treated for more than 2 years were given the option to take a treatment break.
Seven patients chose this option and, so far, none have had evidence on imaging scans that their tumors are growing again.
In December 2022, based on an earlier review of this study and its findings, the Food and Drug Administration approved atezolizumab for adults and children 2 years and older with advanced alveolar soft part sarcoma. This is the first drug ever approved for this rare disease.
“What this trial has shown is that you can manage alveolar soft part sarcoma by managing the immune system,” said Alice Chen, M.D., of NCI’s Division of Cancer Treatment and Diagnosis (DCTD), who led the study. “It’s also possible that patients may be able to stop treatment after a period of time. For these young people, that may make a huge difference.”
“This study is a tour de force,” said Christian F. Meyer, M.D., Ph.D., a sarcoma specialist at Johns Hopkins Medicine, who was not part of the trial. “Eight years ago, we were not thinking about immune therapies for alveolar soft part sarcoma, and here we are now with a drug approval based largely on this work. This study also provides hope that trials in rare cancers are possible and can lead to really pivotal results.”
Although Faithanne had to leave the trial early to undergo a major surgery for her cancer, she said she’s relieved that there is now an approved treatment if her cancer progresses.
“I’m really happy that they’ve found something that works,” she said.
Using immunotherapy to control a rare disease
Alveolar soft part sarcoma, or ASPS, is a type of soft-tissue sarcoma that can form in muscle, bone, nerves, and fat. ASPS grows more slowly than many other sarcomas and generally develops in younger people.
It often starts as a painless lump in the leg, arm, head, or neck but can spread to other parts of the body, such as the lungs. It can also spread to the brain, which is not often seen with other soft tissue sarcomas.
Patients usually have surgery to remove ASPS tumors, often followed by radiation to kill any remaining cancer cells. But the tumors often come back, requiring many subsequent surgeries.
Once the disease spreads beyond where it originally developed, and if the disease spreads to locations where it cannot be surgically removed, there has been no effective treatment for the disease. Less than 50% of people with ASPS that has spread and cannot be treated surgically survive 5 years after diagnosis.
With chemotherapy largely ineffective against ASPS, researchers have been exploring newer treatments, including targeted therapies, but with little success. One targeted therapy, pazopanib (Votrient), has been approved for soft tissue sarcomas in general, but it’s unclear how well it works against ASPS.
Immune checkpoint inhibitors such as atezolizumab have also shown hints of promise. In a small clinical trialExit Disclaimer, tumors shrank in 6 of 11 people with ASPS treated with a combination of the immune checkpoint inhibitor pembrolizumab (Keytruda) and the targeted drug axitinib (Inlyta).
Atezolizumab, which is approved to treat several other types of cancer, had also shown some effectiveness, anecdotally, in several people with this cancer.
Based on these anecdotal findings, Dr. Chen and her colleagues at NCI wanted to see whether they could achieve similar results under the more rigorous standards of a clinical trial. Genentech, which manufactures atezolizumab, provided the drug for the trial under a special research agreement with NCI.
Responses with atezolizumab that appear to last
In the phase 2 trial, 52 adults and children with advanced ASPS who had not previously been treated with checkpoint inhibitors were given an infusion of atezolizumab every 21 days.
Among the 37% of participants whose tumors responded to the treatment, the lone complete response occurred about a year after the person began treatment. Of the remaining 33 participants, 30 had stable disease—that is, their cancer didn’t get better or worse. Typically, without treatment, ASPS tumors will continue to grow, Dr. Chen said.
Most people who responded to treatment began to see tumor shrinkage within the first 3 to 5 months. For three patients, it took more than a year of atezolizumab infusions before their tumors began to shrink.
Side effects of the treatment were mostly mild and included anemia, diarrhea, rash, and pain. Nobody discontinued treatment because of side effects.
After more than 2 years of treatment, seven people opted to take a 2-year break from treatment. Two of the 7 have completed the break without needing to resume atezolizumab at any point, so they have left the study.
The five others are still completing their treatment break. So far, none of the 7 patients have experienced a progression or return of their cancer.
Understanding how atezolizumab works in ASPS
Elad Sharon, M.D., of Dana-Farber Cancer Institute, who co-led the study while he was at NCI, pointed out that atezolizumab has not been shown to be as effective in other sarcomas as it is for ASPS.
Research Team Members

Research Team Members
Designing and running a clinical trial requires the skills of many experts. Each team may be set up differently at different sites. Typical team members and their duties include:
Principal investigator – supervises all aspects of a clinical trial. This person:
- Develops the concept for the trial
- Writes the protocol
- Submits the protocol for the Institutional Review Board (IRB) approval
- Directs the recruitment of patients
- Manages the informed consent process
- Supervises data collection, analysis, interpretation, and presentation
Research nurse – manages the collection of data throughout the course of a clinical trial. This person:
- Educates staff, patients, and referring health care providers about the trial
- Communicates regularly with the principal investigator
- Assists the principal investigator with the informed consent process, study monitoring, quality assurance, audits, and data management and analysis
Data manager – manages the collection of data throughout the course of a clinical trial. This person:
- Enters the data
- Works with the principal investigator and research nurse to identify what data will be tracked
- Provides data to monitoring agencies
- Prepares summaries for interim and final data analysis
Staff physician or nurse – helps take care of the patients during a clinical trial. This person:
- Treats patients according to the clinical trial protocol
- Assesses and records how each patient responds to the treatment and the side effects they may have
- Works with the principal investigator and research nurse to report trends of how patients are doing on the treatment
- Manages each patient’s care
Soft Tissue Sarcoma Pipeline Insight
LAS VEGAS, May 10, 2023 /PRNewswire/ — DelveInsight’s ‘Soft Tissue Sarcoma Pipeline Insight – 2023‘ report provides comprehensive global coverage of available, marketed, and pipeline soft tissue sarcoma therapies in various stages of clinical development, major pharmaceutical companies are working to advance the pipeline space and future growth potential of the soft tissue sarcoma pipeline domain.
Key Takeaways from the Soft Tissue Sarcoma Pipeline Report
- DelveInsight’s soft tissue sarcoma pipeline report depicts a robust space with 125+ active players working to develop 130+ pipeline therapies for soft tissue sarcoma treatment.
- Key soft tissue sarcoma companies such as Advenchen Laboratories, Philogen, Gradalis, Epizyme, Chugai Pharma France, CytRx, Taiho Pharmaceuticals, KaryoPharm Therapeutics, Nanobiotix, Apexigen, Lytix Biopharma, Incyte Corporation, Iovance Biotherapeutics, Aadi Bioscience, Inc., AVEO Pharmaceuticals, Bayer, VasGene Therapeutics, Mirati Therapeutics, Novartis Pharmaceuticals, Incyte Corporation, Tracon Pharmaceuticals, Jiangsu Hengrui Medicine, Exelixis, Qbiotics, AstraZeneca, Loxo Oncology, ImmunityBio, Monopar Therapeutics, Chipscreen Biosciences, Ltd., Agenus, C4 Therapeutics, Inc., Noxopharm Limited, Moleculin Biotech, Inc., Sunshine Guojian Pharmaceutical (Shanghai) Co., Ltd., Tracon Pharmaceuticals Inc., Guangdong Xiangxue Precision Medical Technology Co., Ltd., Cornerstone Pharmaceuticals, Takara Bio Inc., Jazz Pharmaceuticals, Lyell Immunopharma, Telix Pharmaceuticals, and others are evaluating new soft tissue sarcoma drugs to improve the treatment landscape.
- Promising soft tissue sarcoma pipeline therapies in various stages of development include AL-3818, Onfekafusp alfa, Vigil, Tazemetostat, Aldoxorubicin, TAS-116, Selinexor, NBTXR3, APX005M, GPX-150, LTX-315, Lenvatinib, Chiauranib, Zalifrelimab, INCB081776, LN-145-S1, ABI-009, Tivozanib, LOXO-101, sEphB4-HSA, Sitravatinib, Envafolimab, Camrelizumab, Tigilanol Tiglate, Durvalumab, Tremelimumab, CFT8634, NOX66, Liposomal Annamycin, 609A, YH001, TAEST16001, CPI-613+Hydroxychloroquine, TBI-1301, Lurbinectedin, LYL132, and others.
- In October 2022, LIXTE Biotechnology Holdings, Inc. announced that the Spanish Agency for Medicines and Health Products (Agencia Española de Medicamentos y Productos Sanitarios, AEMPS) had authorized a Phase 1b/randomized Phase 2 study of LB-100, the Company’s lead clinical compound, plus doxorubicin versus doxorubicin alone, the global standard for initial treatment of advanced soft tissue sarcomas (ASTS).
- In September 2022, Immutep Limited was pleased to announce it has signed a Material Transfer Agreement (“Agreement”) with the Maria Skłodowska-Curie National Research Institute of Oncology in Warsaw, Poland, to enable an investigator-initiated open-label Phase II clinical trial. The trial will evaluate Immutep’s lead product candidate, efti in combination with pembrolizumab and radiotherapy in the neoadjuvant setting (prior to surgery) in up to 40 patients with select soft tissue sarcoma (STS).
- In September 2022, TRACON Pharmaceuticals, Inc. announced that the U.S. Food and Drug Administration (FDA) has granted fast-track designation for the development of envafolimab (KN035) for patients with locally advanced, unresectable or metastatic undifferentiated pleomorphic sarcoma (UPS) and myxofibrosarcoma (MFS) who have progressed on one or two prior lines of chemotherapy.
- In September 2022, Avacta Group plc announced that the US Food and Drug Administration (FDA) had granted Orphan Drug Designation (ODD) to the company’s lead pre|CISION drug candidate, AVA6000, for treatment of soft tissue sarcoma.AVA6000 is a form of the generic chemotherapy doxorubicin that has been modified using the pre|CISION technology so that it is activated predominantly in the tumor with the aim of sparing healthy tissue from exposure and improving the safety, tolerability, and efficacy of the drug.
- In May 2022, Immix Biopharma, Inc., announced positive interim study data showing that after one cycle of treatment, ImmixBio’s lead candidate IMX-110 produced 75% survival vs. 0% survival for Trabectedin (sold as YONDELIS ® by Janssen, a Johnson & Johnson Company, a U.S. FDA approved drug) in a connective tissue cancer Soft Tissue Sarcoma (STS) mice study. In this study, IMX-110 was compared against approved drugs used to treat STS. Trabectedin was dosed according to Meco et al., 2003 (trabectedin monotherapy treatment arm), and IMX-110 was administered at 2.0 mg/kg.
- In April 2022, Telix Pharmaceuticals Limited announced that it has entered into a license agreement with Eli Lilly and Company (“Lilly”) under which Telix is granted exclusive worldwide rights to develop and commercialize radiolabelled forms of Lilly’s olaratumab antibody for the diagnosis and treatment of human cancers. Telix’s initial development focus will be on a rare type of cancer known as soft tissue sarcoma (STS).
Request a sample and discover the recent advances in soft tissue sarcoma drug treatment @ Soft Tissue Sarcoma Pipeline Report
The soft tissue sarcoma pipeline report provides detailed profiles of pipeline assets, a comparative analysis of clinical and non-clinical stage soft tissue sarcoma drugs, inactive and dormant assets, a comprehensive assessment of driving and restraining factors, and an assessment of opportunities and risks in the soft tissue sarcoma clinical trial landscape.
Soft Tissue Sarcoma Overview
Soft-tissue sarcomas (STS) are rare neoplasms that can develop in supporting or connective tissue, such as muscle, nerves, tendons, blood vessels, and fatty and fibrous tissues. They commonly affect the arms, legs, and trunk. They can also be found in the stomach and intestines (GIST), behind the abdomen (retroperitoneal sarcomas), and in the female reproductive system (gynecological sarcomas). Soft tissue sarcomas are classified based on the cell type involved, the nature of the malignancy, and the clinical course of the disease.
The signs and soft tissue sarcoma symptoms differ greatly between patients depending on the type of soft tissue sarcoma. It is not associated with any obvious symptoms early in the course of the disease, but affected individuals may notice a slow-growing, painless mass in the affected area.
Find out more about drugs for soft tissue sarcoma @ New Soft Tissue Sarcoma Drugs
Learn more about the emerging soft tissue sarcoma pipeline therapies @ Soft Tissue Sarcoma Clinical Trials
Scope of the Soft Tissue Sarcoma Pipeline Report
- Coverage: Global
- Therapeutic Assessment By Product Type: Mono, Combination, Mono/Combination
- Therapeutic Assessment By Clinical Stages: Discovery, Pre-clinical, Phase I, Phase II, Phase III
- Therapeutics Assessment By Route of Administration: Infusion, Intra-arterial, Intradermal, Intralesional, Intratumoral, Intravenous, Oral, Parenteral, Subcutaneous
- Therapeutics Assessment By Molecule Type: Antibody, Antibody-drug conjugate, Cell therapy, Gene therapy, Immunotherapy, Nanoparticle, Peptide, Recombinant fusion protein, Small molecule
- Therapeutics Assessment By Mechanism of Action: Fibroblast growth factor receptor antagonists, Platelet-derived growth factor beta receptor antagonists, Proto oncogene protein c-kit inhibitors, Vascular endothelial growth factor receptor 3 antagonists, Vascular endothelial growth factor receptor-1 antagonists, Vascular endothelial growth factor receptor-2 antagonists, Immunostimulants, Free radical stimulants, DNA intercalators, Type II DNA topoisomerase inhibitors, Cell membrane structure modulators, Antibody-dependent cell cytotoxicity, Programmed cell death-1 receptor antagonists, T lymphocyte stimulants, Type 1 fibroblast growth factor receptor antagonists, Type 3 fibroblast growth factor receptor antagonists, Type 4 fibroblast growth factor receptor antagonists, Type-2 fibroblast growth factor receptor antagonists, Fms-like tyrosine kinase 3 inhibitors, Lymphocyte specific protein tyrosine kinase p56(lck) inhibitors; Lyn protein-tyrosine kinase inhibitors, Src-Family kinase inhibitors
- Key Soft Tissue Sarcoma Companies: Advenchen Laboratories, Philogen, Gradalis, Epizyme, Chugai Pharma France, CytRx, Taiho Pharmaceuticals, KaryoPharm Therapeutics, Nanobiotix, Apexigen, Lytix Biopharma, Incyte Corporation, Iovance Biotherapeutics, Aadi Bioscience, Inc., AVEO Pharmaceuticals, Bayer, VasGene Therapeutics, Mirati Therapeutics, Novartis Pharmaceuticals, Incyte Corporation, Tracon Pharmaceuticals, Jiangsu Hengrui Medicine, Exelixis, Qbiotics, AstraZeneca, Loxo Oncology, ImmunityBio, Monopar Therapeutics, Chipscreen Biosciences, Ltd., Agenus, C4 Therapeutics, Inc., Noxopharm Limited, Moleculin Biotech, Inc., Sunshine Guojian Pharmaceutical (Shanghai) Co., Ltd., Tracon Pharmaceuticals Inc., Guangdong Xiangxue Precision Medical Technology Co., Ltd., Cornerstone Pharmaceuticals, Takara Bio Inc., Jazz Pharmaceuticals, Lyell Immunopharma, Telix Pharmaceuticals, and others.
- Key Soft Tissue Sarcoma Pipeline Therapies: AL-3818, Onfekafusp alfa, Vigil, Tazemetostat, Aldoxorubicin, TAS-116, Selinexor, NBTXR3, APX005M, GPX-150, LTX-315, Lenvatinib, Chiauranib, Zalifrelimab, INCB081776, LN-145-S1, ABI-009, Tivozanib, LOXO-101, sEphB4-HSA, Sitravatinib, Envafolimab, Camrelizumab, Tigilanol Tiglate, Durvalumab, Tremelimumab, CFT8634, NOX66, Liposomal Annamycin, 609A, YH001, TAEST16001, CPI-613+Hydroxychloroquine, TBI-1301, Lurbinectedin, LYL132, and others.
Dive deep into rich insights for new drugs for soft tissue sarcoma treatment; visit @ Soft Tissue Sarcoma Medications
For further information on the soft tissue sarcoma pipeline therapeutics, reach out @ Soft Tissue Sarcoma Drug Treatment
Related Reports
Soft Tissue Sarcoma Market Insights, Epidemiology, and Market Forecast – 2032 report deliver an in-depth understanding of the disease, historical and forecasted epidemiology, market share of the individual therapies, and key soft tissue sarcoma companies, including Gem Pharmaceuticals, Lytix Biopharma, Incyte Corporation, Daiichi Sankyo, NantPharma, Iovance Biotherapeutics, Agenus, Eli Lilly and Company, Adaptimmune, Aadi, AVEO Pharmaceuticals, Amgen, among others.
Soft Tissue Sarcoma Epidemiology Forecast
Soft Tissue Sarcoma Epidemiology Forecast – 2032 report delivers an in-depth understanding of the disease, historical and forecasted epidemiology, as well as the soft tissue sarcoma epidemiology trends.
Clear Cell Sarcoma Pipeline Insight – 2023 report provides comprehensive insights about the pipeline landscape, including clinical and non-clinical stage products and the key clear cell sarcoma companies, including Tesaro, NantPharma, Rafael Pharmaceuticals, Pfizer, among others.
Ewing Sarcoma Pipeline Insight – 2023 report provides comprehensive insights about the pipeline landscape, including clinical and non-clinical stage products, and the key Ewing sarcoma companies, including Gradalis, Inc., Shanghai Pharmaceuticals Holding Co., Ltd, Tyme, Inc, Pfizer, Hutchison Medipharma Limited, among others.
About DelveInsight
DelveInsight is a leading Business Consultant and Market Research firm focused exclusively on life sciences. It supports pharma companies by providing comprehensive end-to-end solutions to improve their performance. Get hassle-free access to all the healthcare and pharma market research reports through our subscription-based platform PharmDelve.
Contact Us
Shruti Thakur
info@delveinsight.com
+1(919)321-6187
www.delveinsight.com
Logo: https://mma.prnewswire.com/media/1082265/DelveInsight_Logo.jpg
SOURCE: PRNewswire
Liquid Biopsies on the Horizon for Children with Solid Cancers

Cancer researchers continue to make progress in developing tests using liquid biopsies that could complement and even serve as an alternative to traditional tissue biopsies. These tests, which analyze bits of free-floating genetic and other material shed by tumors into the blood and other body fluids, are already being used to detect cancer-related genetic changes and guide treatment decisions.
Until recently, much of the research on liquid biopsies focused on their use in adults with cancer. But scientists have begun to make progress in developing liquid biopsy tests specifically for use in children with cancer, including those with solid cancers like Ewing sarcoma, osteosarcoma, and Wilms tumor, a type of kidney cancer.
A recently published study by researchers at Children’s Hospital Los Angeles (CHLA) and the University of Southern California describes the use of one such liquid biopsy approach.
The test, which analyzes bits of DNA in samples of blood, showed promise in diagnosing various types of solid tumors in childrenExit Disclaimer, the team reported February 20 in npj Precision Oncology. It also showed potential for determining whether a tumor is responding to treatment or may be coming back after initial successful treatment.
“It’s a very well done, interesting study and adds a lot of data to the field,” said Mark Applebaum, M.D., a pediatrics researcher at the University of Chicago, who noted that other teams have developed similar approaches. Dr. Applebaum also works in this area but was not involved in the new study.
Liquid biopsies are of particular interest for use in children because they are less invasive and easier to repeat than tissue biopsies, said Jaclyn Biegel, Ph.D., director of the Center for Personalized Medicine at CHLA, who co-led the new study.
The new findings provide “proof of principle” that the test could be useful in the clinic, said Brian Sorg, Ph.D., a program director in NCI’s Cancer Diagnosis Program, who also was not involved in the study.
Challenges of performing biopsies in children
Accurately diagnosing cancer in children can be difficult because children can develop a wide range of solid tumors in different parts of the body. And each tumor type often has multiple subtypes with different features that can affect a patient’s prognosis and treatment, said Miguel Ossandon, Ph.D., also of NCI’s Cancer Diagnosis Program.
A tissue biopsy, in which a sample of tumor is removed with a large needle or during surgery, is still the gold standard for diagnosis, Dr. Ossandon said. “But tissue biopsy has limitations, and some of those limitations can be overcome with a liquid biopsy.”
Some liquid biopsies developed for use in adults with cancer have been approved by the Food and Drug Administration to help guide treatment decisions. But liquid biopsies developed for adults can’t be used for children with cancer.
That’s because “the tumor types you see in children are very different from what you see in adults—the tumors are driven by different genomic [changes],” Dr. Biegel said.
In addition, she said, pediatric liquid biopsies must work with smaller samples of blood or other body fluids.
Liquid biopsy looks for genetic changes typical of pediatric cancers
The liquid biopsy approach that Dr. Biegel and her colleagues developed “is geared towards using very small amounts of DNA” in blood and other body fluids to look for genetic changes typically found in pediatric cancers, she said.
Cancer in adults often results from small changes, or mutations, in one or a few letters (nucleotides) of the DNA code in cells. But solid cancers in children are often caused by changes in the structure of chromosomes in cells, Dr. Biegel explained.
These changes can include the disappearance or duplication of one or more genes in a chromosome, known as copy number alterations. Another common change is a gene fusion, which can result when part of the DNA from one chromosome moves to another chromosome, joining parts of two different genes.
The liquid biopsy test looks for copy number alterations using a technique called low-pass whole-genome sequencing. This method, which can be applied to many samples simultaneously at relatively low cost, can also detect some but not all single-nucleotide changes.
And whereas many liquid biopsies being developed for use in children are designed to detect a single type of cancer, the CHLA and USC team’s approach, as well as similar tests being developed by other researchers, is designed to detect multiple cancer types.
Initial evaluation yields promising results
To evaluate whether their low-pass whole-genome sequencing method could identify the presence of cancer in children known to have the disease and distinguish those with cancer from those without cancer, the team analyzed blood samples from 73 patients with a variety of solid cancers and 19 patients who did not have cancer (controls).
Patients ranged in age from 6 months to 28 years. All cancer patients in the study had a diagnosis that was previously confirmed using established testing methods.
The test successfully detected copy number alterations in DNA from the blood of patients with a range of pediatric solid cancer types, including in 26 of 37 newly diagnosed patients (70%). Of those patients, 27 had localized cancer—that is, the cancer had not spread beyond its original location in the body—and copy number alterations were found in 18 (67%) of them.
The ability to detect copy number alterations in samples from children with localized cancer is noteworthy, Dr. Biegel and her team wrote, because the levels of tumor DNA circulating in blood tend to be lower in patients with localized (earlier-stage) disease.
Of the 19 patients who did not have cancer, 16 did not have detectable copy number alterations. The other three had hereditary losses of a portion of one chromosome that were not related to cancer and were therefore dropped from further analysis.
Next, the team looked at whether their test could detect specific patterns of copy number alterations that are linked with individual cancer types. The test’s ability to do so, they reported, varied depending on the type of cancer.
The researchers also wanted to see if the test has potential to track how childrens’ cancers are responding to treatment or enable earlier detection of cancer that has come back (recurred) after treatment is completed. So, using blood samples taken from patients at different times after treatment, they looked for changes in the levels and patterns of copy number alterations.
In some children, copy number alterations could no longer be detected following treatment, suggesting that the test could be used to monitor patients’ responses to treatment. And in one patient with advanced osteosarcoma, the test detected copy number alterations in blood samples—indicating that the cancer had come back—taken 9 months before imaging tests had shown a recurrence of the cancer.
Since completing this study, Dr. Biegel said that after additional testing, her team has begun using their test for copy number alterations as part of patient care at CHLA and “it’s been extremely helpful,” she said.
For instance, in one patient they used the liquid biopsy to distinguish between two types of childhood liver cancer, hepatoblastoma and a rare cancer called embryonal sarcoma of the liver, that have very different treatments and outlooks.
The team also used the test in samples of cerebrospinal fluid (fluid that circulates around the brain) from some children with brain cancer to help identify cancer that remained after treatment when imaging tests were inconclusive, Dr. Biegel said.
Next version: Additional types of cancer-related changes
The next version of the liquid biopsy test will also look for individual mutations and gene fusions that are well-established markers of certain pediatric cancers using a method known as targeted sequencing. In contrast to low-pass whole-genome sequencing, this method is a deeper dive into one specific region of the genome and more reliably detects these types of genetic changes.
To see if they could detect these changes with a liquid biopsy as effectively as they could using tumor samples, the researchers tested their targeted sequencing approach on blood samples from children with Ewing sarcoma or alveolar rhabdomyosarcoma. They were able to detect cancer-related gene fusions in most patients, including some who did not have detectable copy number alterations.
Both the low-pass whole-genome sequencing and targeted sequencing tests can be done at the same time on a single small sample of blood or other body fluid, Dr. Biegel said.
And, Drs. Ossandon and Sorg said, combining these two tests could improve the performance of the liquid biopsy for detecting and diagnosing childhood cancers.
However, further studies are needed to figure out exactly how and in what cases the combination of these two types of genetic analysis will be most useful, Dr. Biegel said.
She also noted that their liquid biopsy method is not intended as a standalone test but is meant to be combined with other diagnostic methods, such as imaging, when a tissue biopsy is not feasible.
Indeed, like other diagnostic tests, liquid biopsies have both advantages and disadvantages. For instance, Dr. Sorg said, a liquid biopsy can capture genetic material shed by tumors throughout the body, whereas a tissue biopsy “only tells you about the portion of the specific tumor that you’re sampling.”
On the other hand, he continued, a liquid biopsy “doesn’t tell you anything about where the tumors are located,” but that information can usually be obtained with imaging tests.
Before the new test is ready for wider use, Dr. Ossandon said, it will need to be validated in more patients, including children who do not yet have a definitive cancer diagnosis. In addition, he said, clinical trials that follow patients over time will be needed to find out if this and other pediatric liquid biopsy approaches can be used to monitor cancer effectively or provide accurate information on a patient’s prognosis.
“Using low-pass whole-genome sequencing to detect copy number aberrations and [look at] patterns of change over time is a very feasible and doable concept,” Dr. Applebaum said.
“However, we’re still trying to figure out how to use it to guide therapy.”
Tumor microbiome linked to immunotherapy success in sarcoma patients
New UC Davis study finds relationship between tumor microbiome and immune system in patients with soft tissue sarcoma
(SACRAMENTO)In a significant new study, UC Davis Comprehensive Cancer Center researchers have uncovered a link between a patient’s microbiome and their immune system that can potentially be used to improve the treatment of soft tissue sarcoma. This type of cancer is found in connective tissues like muscle, fat and nerves.
Findings from the study were published in the Journal for Immunotherapy of Cancer.
“The study’s data show new lines of research in the paradigm-shifting concept that the microbiome of a patient and their immune system can interact and shape one another, as well as be potentially engineered to improve patient outcomes,” said Robert Canter, the lead author of the study and chief of the Division of Surgical Oncology.
The gut microbiome is made of microorganisms in the digestive tract that include bacteria, fungi and viruses. Microbial communities have also been found in other parts of the body, including the mouth, lungs and skin. And now the study shows they are also found in tumor cells.
“We found that soft tissue sarcomas harbor a quantifiable amount of microbiome within the tumor environment. Most importantly, we found that the amount of microbiome at diagnosis may be linked with the patient’s prognosis,” Canter added.
Although the levels of microbes are low, the study findings are significant because many tumors, especially sarcomas, were believed to be sterile.
“We found that soft tissue sarcomas harbor a quantifiable amount of microbiome within the tumor environment. Most importantly, we found that the amount of microbiome at diagnosis may be linked with the patient’s prognosis.”—Robert Canter, chief, UC Davis Division of Surgical Oncology
Viruses within the microbiome may attract cancer-fighting cells
The UC Davis researchers also uncovered how the microbiome within a sarcoma tumor plays a role in attracting specific types of immune cells like cancer-fighting natural killer cells. Canter said that’s important because the higher the rate of natural killer cell infiltration in a tumor, the greater the chance that the sarcoma won’t spread to other parts of the body. Natural killer cells are a prime target for improving the effectiveness of immunotherapy.
The team found that viruses within the microbiome of a tumor appear to impact the amount of natural killer cells found in sarcomas and, for that reason, affect survival rates. Specifically, the study found a strong positive correlation between the presence of Respirovirus, a genre of viruses known for causing respiratory illnesses, and the presence of natural killer cells in the tumor. Canter and his colleagues are now considering ways to create viruses to attract more cancer-killing immune cells.
“It has become clear that the microbiome in the gut and other parts of the body has a major impact on human health and disease. Amazingly, it shapes the immune system throughout the body and, because of its interaction with the immune system, we now know it also has a big role in how the body responds to cancer and cancer treatments like immunotherapy,” Canter said.
Cross-campus collaboration
The authors obtained tumor and stool samples from 15 adult patients with non-metastatic soft tissue sarcoma, which was studied for a median of 24 months. Analysis revealed that most of the tumors were advanced stage III (87%) and affected a patient’s limb (67%).
Tissue samples were sent to the university’s Genome Center in Davis for sequencing and to the Flow Cytometry Shared Resource Laboratory on the UC Davis medical campus in Sacramento for immune profiling. Patients were monitored for two years as part of their cancer treatment follow-up.
Canter said past research has shown the existence of microbiome inside tumors across several cancer types, including breast, lung, pancreas and melanoma. For that reason, he said further research into the connection between microbiome and the immune system in other cancer types is warranted.
Acknowledgments
Coauthors on the study are Lauren Perry, Sylvia Cruz, Kara Kleber, Sean Judge, Morgan Darrow, Louis Jones, Ugur Basmaci, Nikhil Joshi, Matthew Settles, Blythe Durbin-Johnson, Alicia Gingrich, Arta Monjazeb, Janai Carr-Ascher, Steven Thorpe, William Murphy, and Jonathan Eisen.
This work was supported by the UC Davis Comprehensive Cancer Center and the UC Davis Flow Cytometry Shared Resource Laboratory, with funding from National Cancer Institute grants P30 CA093373, S10 OD018223 and S10 RR 026825. Specimens were provided by the UC Davis Pathology Biorepository, funded by the UC Davis Comprehensive Cancer and the UC Davis Department of Pathology and Laboratory Medicine. The sequencing was carried out at the DNA Technologies and Expression Analysis Cores at the UC Davis Genome Center, supported by National Institutes of Health (NIH) Shared Instrumentation Grant 1S10OD010786-01.
CANCER CARE January 25, 2023
Dexrazoxane Protects the Heart Long Term for Kids Being Treated for Cancer
Today, more than 80% of children diagnosed with cancer are alive 5 years after treatment. This is one of the biggest successes of pediatric medicine in the last 50 years. But the advances in treatment can have a cost: Some childhood cancer survivors develop life-threatening heart problems later in life, due in part to the chemotherapy that initially helped save them.
One of these heart-damaging drugs is doxorubicin (Adriamycin), which is used to treat many types of childhood and adult cancers. Results from a new study show that giving a drug called dexrazoxane (Zinecard) before each dose of doxorubicin substantially decreases the risk that childhood cancer survivors will have treatment-related heart problems in adulthood.
For younger patients, treatment-related heart damage is “an important, life-changing problem because it can impact many decades of life,” said one of the study leaders, Eric Chow, M.D., of the Fred Hutchinson Cancer Center. The study’s findings, he added, have immediate implications for children and teens being treated for cancer today.
The study evaluated the cardiovascular health of 195 people who had been diagnosed with cancer in childhood, about half of whom had received dexrazoxane prior to doxorubicin in clinical trials years earlier.
Almost two decades after their cancer diagnosis, study participants who had received dexrazoxane had healthier hearts than participants who had not received it.
“This has potential to be practice changing,” Dr. Chow said, noting that some doctors have been hesitant to use dexrazoxane without more definitive evidence that it provides long-term protection against heart issues.
Findings from the NCI-funded study were published January 20 in the Journal of Clinical Oncology.
“This is a very important study,” said pediatric oncologist Nita Seibel, M.D., of NCI’s Division of Cancer Treatment and Diagnosis, who was not involved in the work. “We want to make sure childhood cancer survivors have the best quality of life … and anything we can do to prevent heart disease would be beneficial.”
Dexrazoxane offers sustained heart protection two decades out
Heart disease is one of the most concerning long-term side effects from doxorubicin therapy. At least 10% of people who receive high doses of the drug during treatment for childhood cancer experience heart failure by age 40.
Adults with cancer are also at risk of cardiac injury from doxorubicin. In 1995, dexrazoxane was approved by the Food and Drug Administration to reduce the risk of doxorubicin-induced heart damage in women being treated for breast cancer.
In the early 1990s, study co-leader Steven Lipshultz, M.D., chair of the Department of Pediatrics at the University at Buffalo Jacobs School of Medicine and Biomedical Sciences, spearheaded research showing that dexrazoxane could prevent short-term chemotherapy-induced heart damage in children with leukemia. But for years, the drug hasn’t been used widely in children being treated for cancer, Dr. Chow said, due to uncertainties about its long-term risks and benefits.
In the new study, dubbed HEART, participating hospitals in the United States and Canada recruited people who had been treated for childhood cancer at their institutions. The average age of people in the study was 29. All had participated in one of several NCI-supported Children’s Oncology Group or Dana-Farber Cancer Institute Childhood ALL Consortium clinical trials testing dexrazoxane almost 20 years earlier.
Clinicians from the hospitals where study participants were initially treated completed a one-time assessment of each participant’s heart health. That included measuring the structure and pumping strength of the heart’s left ventricle and screening for blood-based markers of heart damage and stress.
Compared with participants who had not received intravenous dexrazoxane prior to doxorubicin, those who received it had significantly better heart-pumping strength, without significant differences in the heart’s ventricular structure. They also had more normal markers of heart muscle stress.
The protection was most notable in those who had received a cumulative dose of doxorubicin greater than 250 mg/m2. This dose is considered to trigger a higher risk for heart disease, according to recently published international guidelines. Dr. Lipshultz emphasized, however, that any child treated with doxorubicin is likely at some risk for future heart problems, regardless of their cumulative dose.
“We found that, 18 years later, the protection to the heart was sustained,” Dr. Lipshultz said.
Importantly, he continued, the new results add to previously reported findings from the same study showing that giving dexrazoxane doesn’t make treatment with doxorubicin less effective against the cancer or increase the likelihood of survivors developing a second primary cancer—a concerning possibility proposed by some doctors.
This is “reassuring,” particularly to the families of children facing treatment with doxorubicin, Dr. Seibel said. “In the past, you would have to say that there is limited long-term data … [so] having longer-term data is definitely better.”
Balancing cancer cures in childhood with decades of active adult life
Doxorubicin is a type of anthracycline. This class of drugs includes many of the most effective chemotherapy drugs for childhood cancers—more than 50% of children with cancer are treated with an anthracycline. But these drugs also harm healthy cells, including heart muscle.
Dr. Lipshultz was one of the first cardiologists to recognize this problem. In the 1980s, he consulted on several cases of childhood cancer survivors who developed heart failure 10 or more years after their cancer diagnosis.
The prevailing thinking at the time was that children who didn’t show evidence of heart failure during treatment were unlikely to have future heart issues, he recalled. But after evaluating more than 100 survivors of childhood cancer who had been treated with doxorubicin, he discovered that more than 60% had unhealthy hearts. This percent, as well as the severity of heart problems for the group, increased over time.
“What we have shown in other studies is that damage occurs with even the very first dose of anthracyclines,” said Dr. Lipshultz, who believes the heart should be protected before every dose.
For 30 years, Dr. Lipshultz has argued that the treatment paradigm for children receiving doxorubicin as part of their cancer treatment needs to shift, noting that the successful treatment of childhood cancer should consider the quality of life for the cancer survivor and their family over a lifespan.
In that sense, these new findings are “so exciting,” Dr. Lipshultz said, because they show we can help prevent long-term damage to the heart from an anthracycline—an effective childhood cancer treatment with an unfortunate side effect.
When an anthracycline enters a cell, it binds to iron, he explained. This creates free radicals that “punch holes” in heart muscle cells and irreversibly damage mitochondria, the energy factories that allow the heart muscle to squeeze with good force, Dr. Lipshultz said. This cell death and mitochondrial damage in childhood leads to an adult heart with weaker muscles, which puts more stress on the heart.
Dexrazoxane, when administered immediately before each doxorubicin infusion, counters this effect by binding up iron in the blood, he continued. In the process, less iron is available to doxorubicin, which decreases the production of free radicals.
Dr. Chow noted that there are factors to consider when using dexrazoxane in children with cancer, such as the potential for a decrease in the production of blood cells in those who are already vulnerable to illness. However, “you can’t give dexrazoxane retroactively,” he said.
Recent guidelines from international organizations recommend dexrazoxane for children receiving certain doses of anthracyclines. Already in the United States, some upcoming treatment guidelines for specific cancers are going to recommend that dexrazoxane be given with any anthracycline dose, Dr. Seibel noted.
More work to be done
The study team acknowledged that the average age of the participants was only 29 years, and clinical heart failure following treatments for childhood cancer may not appear until later. It will be important to follow these patients to see if the lower risk of heart problems becomes more prominent over even longer periods, they wrote.
Dr. Chow noted that most childhood cancer survivors today didn’t receive dexrazoxane prior to their anthracycline treatments. “But rather than despair over that fact, the most important thing for those survivors is trying to control modifiable risk factors for heart disease,” he emphasized. That includes things like maintaining a healthy weight and blood pressure, and controlling diabetes and cholesterol levels.
For now, dexrazoxane is the only heart-protective drug available to children with cancer.
However, some groups are exploring additional protective measures, Dr. Chow said, such as testing a type of anthracycline that has a special fat coating to see if it can stop it from damaging the heart. Other researchers are trying to prevent heart damage by blocking proteins required for the death of heart cells.
Moving forward, this study shows the power of collaborative research involving both oncologists and cardiologists, Dr. Chow said. As a cardiologist, Dr. Lipshultz agreed, saying that he feels privileged to study this generation of long-term survivors of childhood cancer.
Source: National Cancer Institute
Explore other NCI Resources for Sarcomas
What is an Oncology Dietitian?

When you have cancer, your body needs proper nutrients and calories to recover from treatment. Yet, eating well can be difficult when you feel nauseous or don’t have the energy to cook. That’s where an oncology dietitian comes in.
An oncology dietitian (also called an oncology nutritionist) is a key member of your cancer care team. Typically, your oncologist will refer you to an oncology dietitian.
With their extensive background in nutrition, oncology dietitians help you create a meal plan that promotes healing and minimizes side effects while undergoing cancer treatment.
With the help of Melinda Pundt, RDN, LDN, senior dietician nutritionist at the Levine Cancer Institute, we provide more insight into what an oncology dietitian does and how they can support you on your journey to recovery.
What Is the Role of an Oncology Dietitian?
An oncology dietitian works with cancer patients and their families to develop a diet during radiation.
This medical professional helps patients adjust their nutritional intake to optimize health and minimize side effects caused by cancer and cancer treatments.
After gathering more information, your oncology dietitian will develop a nutrition plan with specific food-related goals. This plan will likely include lots of fruits, vegetables, and lean proteins. But it may also include surprising foods like gravy or milkshakes.
Some of the food-related goals within a meal plan are specific to the patient.
For example, if you have experienced dramatic weight loss during chemotherapy, your goal may be to gain 20 pounds. To increase your body mass, your oncology dietitian may offer specific calorie and protein benchmarks.
Your oncology dietitian may also offer:
- Simple, practical tips and advice to help you achieve your nutritional needs
- Advice on ways to deal with weight loss, fatigue, and nausea brought on by illness or treatment side effects
- Personalized guidelines based on your biological needs and unique circumstances
- Plans for families or caregivers in support of your nutritional needs
- Recipes, lists of foods, dietary supplements, and vitamins
- Recommended reading: How to Eat a Healthy Diet During Radiation
Why Is Nutrition Important During Cancer Treatment?
Good nutrition in cancer patients has been linked to better chances of recovery and lower incidences of remission.
A well-rounded diet can also:
- Prevent or combat malnourishment
- Mitigate the deterioration of lean body mass
- Help the patient recover from treatment
- Reduce complications and related illnesses
- Bolster strength and energy
- Increase quality of life
“Your body is constantly having cells damaged from treatment and having cells repair
after treatments,” Pundt offers.
“A balanced diet helps provide your body with the vital vitamins, minerals, protein and energy to help it repair and heal after every treatment.”
Developing a Nutrition Plan With Your Oncology Dietitian
Pundt says that creating a nutritional guide for cancer patients is a delicate balance.
Though the patient needs to consume a diet full of nutrient-dense foods, they also need to eat what tastes good to them.
“Overall, we want the majority of our diet to come from nutrient dense sources, including whole grains, lean protein, healthy fats, vegetables and fruits,” Pundt says.
“But this does not mean every single meal and snack has to be perfectly balanced. Our
comfort foods still provide us with nutrients and joy.”
Many cancer patients are intimidated by oncology nutritionists. They worry that the dietitian will be overly critical of their current diet or suggest they stop eating their favorite foods.
However, your oncology nutritionist is here to support you. Just like how you have a say in choosing your cancer treatment plan, you also have a say in what you eat.
“There are no bad or off-limit foods,” adds Pundt.
“During treatment, your body is using more energy than it would normally. The foods that bring you joy can help with getting in some extra nutrients to support your body during treatments so you can finish treatment on time.”
What To Expect During Your First Consultation
During your first consultation, your oncology nutritionist will perform a physical assessment. Since 85% percent of cancer patients experience malnutrition at some point during radiation treatment, your dietitian will look for fat and muscle loss, thinning hair, brittle nails, and other tell-tale signs of a nutritional imbalance.
The nutritionist will also ask you lots of questions about your diet, like:
- How many meals do you eat per day?
- When do you eat each meal?
- Do you drink soda and other high-sugar beverages?
- What side effects or symptoms are you experiencing?
- Do you experience these symptoms after eating certain foods?
- What are your favorite foods?
- When you feel sick, what do you crave?
“We like to get a feel for our patients’ baseline or normal diet. This can help us identify changes in their diet during treatment,” says Pundt.
“We also like to review any possible nutrition related side effects that patients may experience while undergoing treatment and address these as needed.”
To get the most out of your first dietitian consultation, Pundt suggests that patients:
Make a list of medications, supplements, and vitamins. If you can’t bring all of your bottles with you, take photos.
Note any side effects you are experiencing and when you experience them (e.g. nausea after eating breakfast). Your dietitian may be able to recommend certain foods that will ease symptoms.
Keep a food log for at least a week ahead of time. “Sometimes we aren’t eating as balanced as we may think,” says Pundt. “Food journaling can help you and your dietitian identify if there is anything missing in your diet.”
Any questions you may have. “We want you to be active and present in the management of your health and nutrition,” Pundt says.
What To Expect During Your First Consultation
During your first consultation, your oncology nutritionist will perform a physical assessment. Since 85% percent of cancer patients experience malnutrition at some point during radiation treatment, your dietitian will look for fat and muscle loss, thinning hair, brittle nails, and other tell-tale signs of a nutritional imbalance.
The nutritionist will also ask you lots of questions about your diet, like:
- How many meals do you eat per day?
- When do you eat each meal?
- Do you drink soda and other high-sugar beverages?
- What side effects or symptoms are you experiencing?
- Do you experience these symptoms after eating certain foods?
- What are your favorite foods?
- When you feel sick, what do you crave?
“We like to get a feel for our patients’ baseline or normal diet. This can help us identify changes in their diet during treatment,” says Pundt.
“We also like to review any possible nutrition related side effects that patients may experience while undergoing treatment and address these as needed.”
To get the most out of your first dietitian consultation, Pundt suggests that patients:
Make a list of medications, supplements, and vitamins. If you can’t bring all of your bottles with you, take photos.
Note any side effects you are experiencing and when you experience them (e.g. nausea after eating breakfast). Your dietitian may be able to recommend certain foods that will ease symptoms.
Keep a food log for at least a week ahead of time. “Sometimes we aren’t eating as balanced as we may think,” says Pundt. “Food journaling can help you and your dietitian identify if there is anything missing in your diet.”
Any questions you may have. “We want you to be active and present in the management of your health and nutrition,” Pundt says.
Food Safety During Cancer Treatment
During your consultation, your oncology dietitian will also discuss food safety. Since cancer and cancer treatment can weaken your immune system, it’s important that you avoid food-borne illnesses like salmonella and norovirus.
“Food safety is especially important for those that may have a weakened immune system, like oncology patients. Certain cancer treatments can make it harder for your body to fight off infection so it is important to follow basic food safety rules to lower your risk of getting a food-borne illness,” offers Pundt.
To keep your food safe, your oncology dietitian will recommend:
- Washing your hands before eating
- Keeping surfaces that come into contact with food clean
- Keeping hot foods above 140°F and cold foods below 40°F
- Avoiding cross-contaminating meats and vegetables
- Washing raw fruits and vegetables before consumption
- Avoiding high-risk foods like sushi, undercooked eggs, raw milk or cheese, raw sprouts, and self-serve buffets
Source: SERO
FDA grants approval to atezolizumab for alveolar soft part sarcoma
On December 9, 2022, the Food and Drug Administration (FDA) approved atezolizumab (Tecentriq, Genentech, Inc.) for adult and pediatric patients 2 years of age and older with unresectable or metastatic alveolar soft part sarcoma (ASPS).
Details of the FDA Approval
Efficacy was evaluated in Study ML39345 (NCT03141684), an open-label, single-arm study in 49 adult and pediatric patients with unresectable or metastatic ASPS. Eligible patients were required to have histologically or cytologically confirmed ASPS incurable by surgery and an ECOG performance status of ≤2. Patients were excluded for primary central nervous system (CNS) malignancy or symptomatic CNS metastases, clinically significant liver disease, or a history of idiopathic pulmonary fibrosis, pneumonitis, organizing pneumonia, or active pneumonitis on imaging. Adult patients received 1200 mg intravenously and pediatric patients received 15 mg/kg (up to a maximum of 1200 mg) intravenously once every 21 days until disease progression or unacceptable toxicity.
The main efficacy outcome measures were overall response rate (ORR) and duration of response (DOR) determined by an independent review committee using RECIST v1.1. ORR was 24% (95% CI: 13, 39). Of the 12 patients who experienced an objective response, 67% had a DOR of 6 months or more, and 42% had a DOR of 12 months or more.
The median patient age was 31 years (range: 12-70); 47 adult patients (2% were ≥65 years of age) and 2 pediatric patients ≥12 years of age were enrolled; 51% were female, 55% White, 29% Black or African American, 10% Asian.
The most common adverse reactions (≥15%) were musculoskeletal pain (67%); fatigue (55%); rash (47%); cough (45%); nausea, headache, and hypertension (43% each), vomiting (37%), constipation and dyspnea (33% each), dizziness and hemorrhage (29% each), insomnia and diarrhea (27% each), pyrexia, anxiety, abdominal pain and hypothyroidism (25% each), decreased appetite and arrhythmia (22% each), influenza-like illness and weight decreased (18% each), and allergic rhinitis and weight increased (16% each).
The recommended atezolizumab dosage for adult patients is 840 mg every 2 weeks, 1200 mg every 3 weeks, or 1680 mg every 4 weeks until disease progression or unacceptable toxicity. The recommended dosage for pediatric patients 2 years of age and older is 15 mg/kg (up to a maximum of 1200 mg) every 3 weeks until disease progression or unacceptable toxicity.
View full prescribing information for Tecentriq.
This review used the Assessment Aid, a voluntary submission from the applicant to facilitate the FDA’s assessment. The FDA approved this application 3 weeks ahead of the FDA goal date.
This application was granted priority review and breakthrough designation. A description of FDA expedited programs is in the Guidance for Industry: Expedited Programs for Serious Conditions-Drugs and Biologics. The application also was granted orphan drug designation.
Healthcare professionals should report all serious adverse events suspected to be associated with the use of any medicine and device to FDA’s MedWatch Reporting System or by calling 1-800-FDA-1088.
For assistance with single-patient INDs for investigational oncology products, healthcare professionals may contact OCE’s Project Facilitate at 240-402-0004 or email OncProjectFacilitate@fda.hhs.gov.
Source: FDA
Announcing Our 2022 Sarcoma Research Grant

The Paula Takacs Foundation is proud to announce its 2022 sarcoma research grant in the amount of $275,000 to Levine Cancer Institute and Levine Children’s Hospital. This grant is an organizational record thanks to our very passionate and dedicated supporters and volunteers!
Behind the Scenes of the 2022 Research Grant
“2022 was an outstanding year for our foundation!” said Susan Udelson, Executive Director. “During our signature fundraiser, The Sarcoma Stomp, presented by AmWINS, dedicated fundraisers and donors fired on all cylinders, and companies supported in droves. We held Golf Fore Sarcoma in the fall and gained many new and generous supporters. We also had the great fortune of benefiting from several other fundraisers this year: All-In to Fight Cancer’s Texas Hold’em tournament, Food & Beverage Social Club’s FORK Cancer chef’s dinner, and the Bakerstrong golf tournament in memory of Clayton Baker, hosted by his friends and Ernst & Young colleagues. We are extremely grateful to these partners who helped us amplify our impact.”
On December 6, 2022 the Paula Takacs Foundation for Sarcoma Research held a Gift Presentation and Reception for Levine Cancer Institute, Levine Children’s Hospital and other guests. It was sponsored by and held at Loretta’s Restaurant in Charlotte, NC. We thank Loretta’s Restaurant for supporting our mission!
Research Grant and Donor Impact
The Paula Takacs Foundation donors have funded a pilot study of a sarcoma-specific blood biopsy technique developed by Levine Cancer Institute. Researchers now report that the preliminary data is extremely encouraging! This study has found evidence of circulating tumor DNA of several sarcoma subtypes in the blood. This has the potential to be a game changer for more effective patient management and a better understanding of sarcoma drivers.
Donations have also supported Levine researchers in the study of genomic sequencing of over 70 synovial sarcoma specimens and comparing to patient outcomes. Although not yet published, this is currently the largest study of synovial sarcoma in the world! It is very significant to amass a large study in a very rare disease. It helps researchers uncover the drivers of this disease and gives patients so much hope for a cure.
Read about all the studies your dollars fund.
Our New Program is Revealed!
The Foundation is also proud to announce a new initiative. Through the Growing Hope Through Art program, a fundraising arm the Paula Takacs Foundation, we will knit together our community in awareness and purpose about sarcomas. Powerful art installations commissioned by the Program will stand as a symbol of our commitment to funding local research, and amplifying awareness as they tell stories of hope throughout the Charlotte region. The first installation, by glass artist Jake Pfeifer of Hot Glass Alley, will be in a prominent corridor at Levine Cancer Institute. Seasons of Life, a hand-blown glass tree with a seasonal cadence of blossoms, will symbolize the courageous sarcoma journey of the artist, and will pay homage to all cancer patients and their healthcare heroes.
To learn more, visit growinghopethroughart.org.
How Can You Help Make the 2023 Research Grant Even Larger?
There are many ways to get involved in the work of the Paula Takacs Foundation! To learn more, you can visit our website, follow us on Instagram and Facebook, and opt in to our periodic email updates. We need YOU to help fund the research that can lead to cures, and to spread awareness that can lead to faster diagnoses in order to save more lives!
Subscribe to our mailing list HERE and receive our newsletters.
Changing the Perception of Early-Phase Cancer Clinical Trials: A Conversation with Dr. Naoko Takebe

Clinical trials are an indispensable step in moving new cancer treatments from laboratory discoveries into everyday patient care. The initial human studies of new cancer treatments are called phase 1 clinical trials, and their primary goal is to find a safe dose for further testing. But a recent analysis shows that, despite their focus on safety, phase 1 trials of new cancer treatments may benefit participants more than previously thought.
In the analysis, Naoko Takebe, M.D., Ph.D., of NCI’s Cancer Therapy Evaluation Program (CTEP), and her NCI colleagues surveyed the last two decades of phase 1 clinical trials for solid tumors sponsored by CTEP. Over that period, they found, the number of trial participants whose tumors shrank or disappeared nearly doubled and the percentage of patients whose tumors stopped growing for a time also increased. The risk of death caused by a new treatment being tested, however, remained steady and very low, at less than 1%.
In this interview, Dr. Takebe talks about the findings and how they may alter the perception of these important early-phase trials.
Do you feel like there are misconceptions about phase 1 clinical trials?
Yes, the perception of the potential benefit to patients hasn’t caught up with modern drug development. In the past, participants in phase 1 trials generally have had low tumor response rates, about 4%–5%. In addition, the primary purpose of phase 1 trials is to assess safety. So, some doctors have not been enthusiastic about referring patients to phase 1 trials.
People also have to go through the standard treatment options first, and usually only those patients who run out of those options, or are not able to receive those standard options for some reason, are eligible to participate in a phase 1 trial. So there have been concerns about including people with advanced cancer, who may be very ill, in early clinical trials.
But we and others have now shown that things have changed. Participating in phase 1 trials has more potential for clinical benefit than is commonly believed, largely due to the development of modern cancer drugs, like targeted therapies, immunotherapies, and new combination therapies.
So I hope this analysis will have a positive impact on the enrollment of patients into phase 1 trials by doctors, who may feel more comfortable referring patients.
You found a few groups of people who had a slightly higher risk of treatment-related death in phase 1 trials compared with participants overall, including those who were older and sicker, and who had liver problems. Should these people not participate in clinical research?
No, they can definitely still participate, as long as they meet all the criteria for participation in a trial, and their doctor agrees it’s safe. And we have to overcome the misperception that they can’t.
In addition to the newer types of drugs being developed, we’ve also had advancements in supportive care. In all clinical trials, we’re now much more proactive in supporting patients, including providing pain control and palliative care services, and watching for and appropriately managing side effects.
So factors like age should not necessarily stop patients from participating in a phase 1 clinical trial. But they should serve as an alert for the clinical trial team to be aware, to make sure patients understand the risks, and to monitor older, sicker patients more closely.
What other factors should patients and their doctors consider when weighing participation in a phase 1 clinical trial?
Participation in phase 1 trials does pose both a time and logistical burden, because there are frequent safety assessments on top of other aspects of treatment. Some patients may want more time at home with their families, rather than going back and forth between appointments.
But in order for patients to make an informed decision, we believe those with no further standard treatment options for their cancer should be informed about the option of participating in phase 1 trials.
“First-in-human” studies that test new drugs are just one type of phase 1 trial. Can you explain what other types of phase 1 trials are available, if people feel uncomfortable about the idea of participating in a first-in-human study?
Trials testing the safety and tolerability of a new drug for the first time in people are mostly sponsored by pharmaceutical companies. NCI sponsors some first-in-human phase 1 trials, but they’re not that common.
NCI tends to sponsor phase 1 trials investigating new combinations of drugs. Even if the drugs being used together have been tested individually in people, they are also required to be tested together in a phase 1 trial to determine the optimal dose of each agent that can be given safely in combination.
About 70% of the clinical trials that we analyzed in this study were drug combination trials.
How will greater participation in phase 1 trials benefit cancer medicine in general?
Enrollment in phase 1 trials has tended to be very slow. If we can enroll more patients more quickly, we can do additional phase 1 studies and ultimately bring more new drugs to patients faster.
But for more referrals, we hope oncologists will view these recent findings as paradigm shifting, and to have discussions with their patients about the potential benefit of participating in a phase 1 clinical trial, alongside the opportunity to advance cancer research.
The patients ultimately decide whether they should participate, but we, the oncologists, have to give them that option.
Source: National Cancer Institute, Cancer Currents Blog
Photo Credit: iStock
Steps to Find a Clinical Trial

Want to Find a Clinical Trial?
If you are thinking about joining a clinical trial as a treatment option, the best place to start is to talk with your doctor or another member of your health care team. Often, your doctor may know about a clinical trial that could be a good option for you. He or she may also be able to search for a trial for you, provide information, and answer questions to help you decide about joining a clinical trial.
Some doctors may not be aware of clinical trials that could be appropriate for you. If so, you may want to get a second opinion about your treatment options, including taking part in a clinical trial.
If you decide to look for trials on your own, the steps discussed here can guide you in your search. The NCI‘s Cancer Information Service can also provide a tailored clinical trials search that you can discuss with your doctor. To reach them call 1-800-4-CANCER (1-800-422-6237) and select option 2. This is a free service. Keep in mind that the search results do not replace advice from your doctor.
Step 1: Gather details about your cancer
If you decide to look for a clinical trial, you will need to know certain details about your cancer diagnosis and compare these details with the eligibility criteria of any trial that interests you. Eligibility criteria are the requirements that must be met for you to join a clinical trial.
Examples of eligibility criteria include
- having a certain type or stage of cancer
- having received (or not having received) a certain type of treatment in the past
- having specific genetic changes in your tumor
- being in a certain age group
- medical history
- current health status
To help you gather details about your cancer, complete as much of the Cancer Details Checklist as possible. Refer to the form during your search for a clinical trial.
If you need help filling out the form, talk with your doctor or nurse or social worker at your doctor’s office. The more information you can gather, the easier it will be to find a clinical trial to fit your situation.
Step 2: Find clinical trials
There are many lists of cancer clinical trials taking place in the United States. Some trials are funded by nonprofit organizations, including the U.S. government. Others are funded by for-profit groups, such as drug companies. Hospitals and academic medical centers also sponsor trials conducted by their own researchers. Because of the many types of sponsors, no single list contains every clinical trial.
Helpful tip: Whichever website you use to search for clinical trials, be sure to bookmark or print a copy of the protocol summary for every trial that interests you.
A protocol summary should explain the goal of the trial and describe which treatments will be tested. It should also list the locations where the trial is taking place.
Keep in mind that protocol summaries are written for health care providers and use medical language to describe the trial that may be difficult to understand. For help understanding the protocol summary, call, email, or chat with one of our cancer information specialists.
NCI-supported clinical trials
NCI’s website helps you find NCI-supported clinical trials that are taking place across the United States, Canada, and internationally. The list includes
- All NCI network trials, including trials supported through the
- Trials that are funded in full or in part by NCI, including trials taking place at NCI-Designated Cancer Centers
- Trials at the NIH Clinical Center in Bethesda, Maryland
If you need help with your search, you can call, email, or chat with one of our trained information specialists. They will need to know details about your cancer, so have your Cancer Details Checklist ready.
Other lists of clinical trials
In addition to NCI‘s list of cancer clinical trials, you may want to check a few other lists.
ClinicalTrials.gov
ClinicalTrials.gov, which is part of the National Library of Medicine, lists clinical trials for cancer and many other diseases and conditions. It contains trials that are on NCI’s list of cancer trials as well as trials sponsored by pharmaceutical or biotech companies that may not be on NCI’s list.
Cancer centers and clinics that conduct cancer clinical trials
Many cancer centers across the United States, including NCI-Designated Cancer Centers, sponsor or take part in cancer clinical trials. The websites of these centers usually have a list of the clinical trials taking place at their institutions. Some of the trials included in these lists may not be on NCI’s list.
Keep in mind that the amount of information about clinical trials on these websites can vary. You may have to contact a cancer center clinical trials office to get more information about the trials that interest you.
Drug and biotechnology companies
Many companies provide lists of the clinical trials that they sponsor on their websites. Sometimes, a company’s website may refer you to the website of another organization that helps the company find patients for its trials. The other organization may be paid fees for this service.
Clinical trial listing services
Some organizations provide lists of clinical trials as a part of their business. These organizations generally do not sponsor or take part in clinical trials. Some of them may receive fees from drug or biotechnology companies for listing their trials or helping find patients for their trials.
Keep the following points in mind about clinical trial listing services
- The lists of trials provided by these organizations often draw from the trial lists that are available from the United States government (NCI and ClinicalTrials.gov).
- The websites of these organizations may not be updated regularly.
- The websites of these organizations may require you to register to search for clinical trials or to obtain trial contact information for trials that interest you.
Cancer advocacy groups
Cancer advocacy groups provide education, support, financial assistance, and advocacy to help patients and families who are dealing with cancer, its treatment, and survivorship. These organizations recognize that clinical trials are important to improving cancer care. They work to educate and empower people to find information and obtain access to appropriate treatment.
Advocacy groups work hard to know about the latest advances in cancer research. Some will have information about clinical trials that are enrolling patients.
To find trials, search the websites of advocacy groups for specific types of cancer. Many of these websites have lists of clinical trials or refer you to the websites of organizations that match patients to trials. Or, you can contact an advocacy group directly for help finding clinical trials.
Step 3: Take a closer look at the trials that interest you
Once you have completed the Cancer Details Checklist and found some trials that interest you
- Take a closer look at the protocol summary for each trial.
- Use the questions below to narrow your list to include only those trials for which you would like to get more information.
Helpful tip: Don’t worry if you can’t answer all of the questions below just yet. The idea is to narrow your list of potential trials, if possible. However, don’t give up on trials you’re not sure about. You may want to talk with your doctor or another health care team member during this process, especially if you find the protocol summaries hard to understand.
Key questions to ask about each trial:
Trial objective
What is the main purpose of the trial? Is it to cure your cancer? To slow its growth or spread? To lessen the severity of cancer symptoms or the side effects of treatment? To determine whether a new treatment is safe and well-tolerated? Read this information carefully to learn whether the trial’s main objective matches your goals for treatment.
Eligibility criteria
Do the details of your cancer diagnosis and your current overall state of health match the trial’s eligibility criteria? Some treatment trials will not accept people who have already been treated for their cancer. Other treatment trials are looking for people who have already been treated for their cancer.
Helpful tip: If you have just found out that you have cancer, the time to think about joining a trial is before you have any treatment. Talk with your doctor about how quickly you need to make a treatment decision.
Trial location
Is the location of the trial manageable for you? Some trials take place at more than one location. Look carefully at how often you will need to receive treatment during the course of the trial. Decide how far and how often you are willing to travel. You will also need to ask whether the sponsoring organization will pay for some or all of your travel costs.
Study length
How long will the trial run? Not all protocol summaries provide this information. If they do, consider the time involved and whether it will work for you and your family.
After thinking about these questions, if you are still interested in a clinical trial, then you are ready to contact the team running the trial.
Step 4: Contact the team running the trial
There are a few ways to reach the clinical trial team.
- Contact the trial team directly. The protocol summary should include the phone number of a person or an office that you can contact for more information. You do not need to talk to the lead researcher (called the “protocol chair” or “principal investigator“) at this time, even if his or her name is given along with the telephone number. Instead, call the number and ask to speak with the “trial coordinator.” This person can answer questions from patients and their doctors. It is also the trial coordinator’s job to decide whether you are likely to be eligible to join the trial. However, a final decision will probably not be made until you have met with a doctor who is part of the trial team.You will need to refer to the Cancer Details Checklist during this conversation, so keep it handy.
- Ask your doctor or another health care team member to contact the trial team for you. The clinical trial coordinator will ask questions about your cancer diagnosis and your current general health that you may not be sure how to answer. So, you may want to ask your doctor or someone else on your health care team to contact the trial coordinator for you.
- The trial team may contact you. If you have registered to use the website of a clinical trial listing service and found a trial that interests you, the clinical trial team may contact you directly by using the phone number and email address you provide when you register.
Step 5: Ask questions
Whether you or someone from your health care team speaks with the clinical trial team, this is the time to get answers to questions that will help you decide whether or not to take part in this particular clinical trial. Questions to Ask Your Doctor about Treatment Clinical Trials can help you think about questions you want to ask.
Remember to keep your Cancer Details Checklist handy to help you answer some of the questions that may be asked.
Talk with your doctor
To make a final decision, you will want to know the potential risks and benefits of all treatment options available to you. If you have any remaining questions or concerns, you should discuss them with your doctor. Ask your doctor some of the same questions that you asked the trial coordinator. You should also ask your doctor about the risks and benefits of standard treatment for your cancer. Then, you and your doctor can compare the risks and benefits of standard treatment with those of treatment in a clinical trial. You may decide that joining a trial is your best option, or you may decide not to join a trial. It’s your choice.
Step 6: Make an appointment when you find a clinical trial
If you decide to join a clinical trial for which you are eligible, schedule a visit with the team running the trial.
Source: National Cancer Institute
New Cancer Model Shows Promise in Predicting If Treatment Will Shrink Tumors
Will a specific cancer treatment actually work for a person diagnosed with cancer? Every person’s cancer is different, and even when a tumor has a genetic change for which there’s a matching targeted therapy, there’s no guarantee a given treatment is going to work.
But based on the results of a small study, funded in part by NCI, a team of researchers hopes to soon offer oncologists a new tool to guide treatment choices for their patients.
The tool is a new type of personalized tumor model, called micro-organospheres. And in a small study of eight people with advanced colorectal cancer, the researchers used the model to accurately predict whether the chemotherapy drug oxaliplatin would shrink their tumors.
Results from the study, led by Xiling Shen, Ph.D., the CEO of the biotechnology company Xilis, were reported June 2 in Cell Stem Cell.
To create the micro-organospheres, the research team takes tissue from a patient’s tumor biopsy and runs it through a desktop device, about the size of a standard printer. The end product: thousands of three-dimensional mini-replicas of the cancer suspended in tiny compartments on a lab dish.
Creating the models required much less tumor tissue than is usually required to grow other cancer models that use a patient’s own tumor tissue, Dr. Shen and his colleagues reported. And they were created quickly, in less than 2 weeks. That is much faster than similar models can be created, explained one of the study’s leaders, David Hsu, M.D., Ph.D., of the Duke Cancer Institute.
Their analyses also showed that the micro-organospheres largely retained the molecular features of the tumors from which they were created. And the models had many other components of the tumor’s surroundings, including immune cells and structural cells. The makeup of this tumor “microenvironment,” as it’s called, can influence how tumors respond to treatment.
The micro-organospheres “overcome a lot of the barriers” that have prevented similar tumor models from being used to help direct everyday patient care, Dr. Hsu said.
A larger study is being launched to determine whether these early findings hold up. Dr. Shen and Dr. Hsu, along with a third member of the team, Hans Clevers, M.D., Ph.D., of the pharmaceutical company Roche and a pioneer in organoid technology, jointly founded Xilis in 2019 to commercialize the technology.
The findings from this first study “are just a proof of concept,” Dr. Hsu acknowledged. “We need a larger study to … have the data needed to say if [these models] precisely capture patients’ response to treatment.”
From PDX and organoids to micro-organospheres
Cancer models, including tumor cell lines and animal models, are widely used research tools. They usually serve as generalized stand-ins for a specific type or form of cancer.
But over the past decade, researchers have taken these representations of cancer to the next level, developing personalized models created from individual patients’ tumor tissue. Efforts to create these patient-derived tumor models, as they’re called, are considered to be an important part of a concept known as precision oncology: treating a patient’s cancer based on its unique clinical and molecular features.
The two most common patient-derived models are mouse models called patient-derived xenografts (PDXs) and tumor-like cell clusters called organoids that are grown in lab dishes.
Because they grow as human tumors in living tissue, there was initially great hope that PDXs might be used to direct care for individual patients, explained Konstantin Salnikow, Ph.D., of NCI’s Division of Cancer Biology and who oversees NCI’s Patient-Derived Models of Cancer program.
But it soon became clear that because of certain limitations, in their current forms, PDX models may primarily be most useful as research tools and not to help direct the care of individual patients, Dr. Salnikow said.
Those limitations include the time it takes to establish them—a minimum of several months, and “sometimes up to a year,” Dr. Salnikow said. And because PDX mice lack functioning immune systems, he added, they can’t capture the important interactions between immune cells and tumors, which can influence how cancer treatments work.
Organoids, which are created using specific types of stem cells in tumor tissue, are grown in laboratory dishes. These models can be created somewhat more quickly and inexpensively than PDX models.
But when it comes to cancer, treatment typically needs to begin quickly after diagnosis, usually within a few weeks, said Dr. Hsu, who specializes in treating colorectal cancer.
Not only does creating organoids require a relatively large amount of tumor tissue—which isn’t always easy to come by—it also can take several months. In addition, the number of organoids produced is relatively small. For the time being, these factors may limit their potential for use in everyday patient care, he explained.
Micro-organospheres are intended to address both models’ limitations.
An electrical engineer by training, Dr. Shen developed the system for creating micro-organospheres at Duke. He recently left the university to lead Xilis full time.
The system’s lynchpin is a technology called microfluidics, which allows for precise handling of very small amounts of material suspended in specialized liquids. Producing the micro-organospheres also involves growing the collected cells in oil-based droplets, which required the researchers to develop a way to then remove the oil without harming the cells.
The entire process is highly automated and takes place in a small, desktop device. By automating production, the system eliminates much of the variability involved in growing organoids, which requires multiple manual steps, and streamlines the entire process, Dr. Shen explained.
As a result, he continued, there won’t be “different results depending on who cultured [the] cells.”
And rather than a just few organoids or PDXs, the product that emerges from the system is “thousands of miniaturized tumors,” Dr. Shen said, “and those mini-tumors are ready for drug testing within days.”
Source: National Cancer Institute
Photo Credit: Image used courtesy of Xiling Shen
Four multinational, interdisciplinary teams selected to address major challenges in cancer

The Cancer Grand Challenges program will award $100 million to four interdisciplinary teams from around the world to solve some of the toughest challenges in cancer research. Each team will receive $25 million over five years. The teams were announced at the Cancer Grand Challenges Summit on June 16, 2022, in Washington, D.C.
The National Cancer Institute (NCI) and Cancer Research UK, the world’s leading funders of cancer research, partnered to launch the Cancer Grand Challenges program. Cancer Grand Challenges aims to provide multiple rounds of funding for interdisciplinary research teams from around the world whose novel ideas have the greatest potential to advance cancer research and improve outcomes for people affected by cancer.
4 Interdisciplinary Teams
The research being conducted by the four selected interdisciplinary teams includes investigation of 1) a muscle-wasting condition in cancer patients known as cachexia, 2) the biology of extrachromosomal DNA in cancer 3) new therapies for solid tumors in children, and 4) what triggers normal cells harboring cancer-causing mutations to become tumor cells.
“The partnership with Cancer Research UK to develop the projects funded for the Cancer Grand Challenges program will enable a global collaboration on a disease that has touched everyone around the world,” said Douglas R. Lowy, M.D., acting director of NCI. “We’re confident these multidisciplinary teams of scientists — with the flexibility and scale to innovate and carry out cutting-edge research — will be able to address several critical cancer research problems that can advance the understanding of cancer and benefit patients.”
“Cancer is a global issue that demands global collaboration. By investing in team science at this scale, we will bring new thinking to problems that have, for too long, stood in the way of progress,” said David Scott, Ph.D., director of Cancer Grand Challenges, Cancer Research UK. “At its core, Cancer Grand Challenges provides multidisciplinary teams the time, space, and freedom to innovate and drive progress against cancer that the world urgently needs. The new teams join a growing global community already making major discoveries, including unlocking new information about the tumor microenvironment and transforming our understanding of the early stages of disease development.”
A total of 169 research teams from more than 60 countries submitted preliminary proposals outlining how they would tackle one of the nine challenges posed by the Cancer Grand Challenges program. From those submissions, 11 teams were chosen by an expert group — which included input from a patient committee — to receive seed funding to develop their ideas into full proposals. Four funded teams, representing four of the challenges, were selected from those proposals.
The winning interdisciplinary teams (by their chosen names) and challenges
- The CANCAN team will explore cancer cachexia as a tumor-driven syndrome. Cachexia is a debilitating muscle wasting syndrome that dramatically affects quality of life and survival for many people with advanced cancer. The team is led by Eileen White, Ph.D., Rutgers Institute of New Jersey; Marcus DaSilva Goncalves, M.D., Ph.D., Weill Cornell Medicine, New York City; and Tobias Janowitz, M.D., Ph.D., Cold Spring Harbor Laboratory, New York.
- The eDyNAmiC team seeks to understand the creation and action of extrachromosomal DNA (ecDNA), which helps tumors evolve and evade treatment. They are also developing new ways to target these mechanisms in cancer. The team is led by Paul Mischel, M.D., Stanford University.
- The NexTGen team will work to develop engineered T-cell therapies for childhood cancer. They will also explore whether changing the tumor microenvironment can help make treatments more effective. The team is led by Catherine Bollard, M.D., Children’s National Hospital, Washington, D.C.; and Martin Pule, University College London.
- The PROMINENT team aims to discover what triggers normal cells to become cancerous to inform prevention. They will explore how carcinogens and other mutation-forming factors help turn a normal cell into a tumor cell. The team is led by Allan Balmain, Ph.D., University of California San Francisco; Paul Brennan, Ph.D., International Agency for Research on Cancer; and Núria López Bigas, Ph.D., Institute for Research in Biomedicine Barcelona.
“Through this unique partnership, Cancer Grand Challenges fosters scientific creativity of the highest order, giving priority to innovative ideas that are beyond what can be supported through more traditional mechanisms,” said Dinah S. Singer, Ph.D., NCI deputy director for scientific strategy and development.
The next funding rounds of the NCI-Cancer Research UK partnership are planned for 2023 and 2025. For more information about the Cancer Grand Challenges program, visit https://www.cancer.gov/cancer-grand-challenges.
About the National Cancer Institute (NCI): NCI leads the National Cancer Program and NIH’s efforts to dramatically reduce the prevalence of cancer and improve the lives of cancer patients and their families, through research into prevention and cancer biology, the development of new interventions, and the training and mentoring of new researchers. For more information about cancer, please visit the NCI website at or call NCI’s contact center, the Cancer Information Service, at 1-800-4-CANCER (1-800-422-6237).
About the National Institutes of Health (NIH): NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit nih.gov.
100% Complete Response Rate in Rectal Cancer Clinical Trial

Breakthrough findings were presented at the 2022 ASCO Annual Meeting and published in The New England Journal of Medicine today by researchers at Memorial Sloan Kettering Cancer Center (MSK) confirming a clinical complete response in all 14 patients who received the immunotherapy treatment dostarlimab as a first-line treatment for mismatch repair-deficient (MMRd) locally advanced rectal cancer. This new approach of “immunoablative” therapy uses immunotherapy to replace surgery, chemotherapy and radiation to remove cancer.
MSK’s Andrea Cercek, MD, Section Head of Colorectal Cancer and Co-Director of the Center for Young Onset Colorectal and Gastrointestinal Cancer, and Luis Alberto Diaz, Jr., MD, Head of the Division of Solid Tumor Oncology, led this groundbreaking clinical trial — which saw a 100% complete response rate among its patients. The study also provides a framework for evaluation of highly active therapies in the neoadjuvant setting, where patients are spared from chemoradiation and surgery while treating the tumor when it is most likely to respond.
Rectal Cancer Study Details and Findings
“Since MMRd colorectal cancer is responsive to PD-1 blockade in the metastatic setting, we hypothesized that locally advanced mismatch repair-deficient rectal cancer is sensitive to checkpoint blockade and may alter the requirements for chemoradiotherapy and surgery, or eliminate the need for additional treatments altogether,” explained Dr. Cercek.
MSK researchers conducted a prospective study in which single agent dostarlimab, an anti-PD-1 monoclonal antibody, was administered every three weeks for six months in patients with mismatch repair-deficient stage 2 and 3 rectal adenocarcinoma, to be followed by standard chemoradiation and surgery. Patients who achieved a clinical complete response were eligible for omission of chemoradiation and surgery.
All 14 who initiated treatment on the trial and have had at least six months of follow-up achieved a clinical complete response with no evidence of tumor on MRI, FDG-PET, endoscopic visualization, digital rectal exam, or biopsy, which satisfied the study’s co-primary endpoint. To date, no patients have required chemoradiation or surgery, and no cases of progression or recurrence have been noted during follow-up (up to 25 months). No serious adverse events were observed. As researchers found the elimination of tumors following six months of therapy with PD-1 blockade, it enabled them to omit both chemoradiation and surgery and to proceed with observation alone.
Cancer experts hail a molecular ‘black box’ that records how cells fly into tumor territory
Biologists Tyler Jacks and Jonathan Weissman’s mice may look like any other lab mice — plain, pale, and furry — but cancer geneticists see them as a “technical tour de force.”
“It’s a pretty heavily engineered mouse,” said Weissman, a biologist at the Whitehead Institute.
Cancer experts find molecular ‘black box’
Engineered into that mouse is intricate molecular machinery that allowed Weissman and his team to trace the ancestries of single tumor cells, placing them on a tumor’s family tree with an unprecedented level of detail. With those findings, scientists say that Weissman, in a new paper published this month, has begun to uncover new insights into the fundamental biology of tumors and how they evolve.
“It’s like a molecular flight recorder like the black box on a plane,” Weissman said. With this technology, developed by his lab and others, “you can reconstruct the history of how a tumor evolved and became aggressive, even try to understand the vulnerabilities that a tumor has at a very early stage.”
The detailed tumor evolution in the study is something that’s completely new to cancer research, said Kamila Naxerova, a systems biologist at Massachusetts General Hospital who studies tumor evolution and was not involved with the work. “There’s no comparison,” said Naxerova, one of several outside experts who called the work a tour de force. “This is something now uniquely enabled by the methods they used here — how different cancer cell states change over time as the tumor lineage evolves? There’s no prior data.”
Experts watch mutations form
Malignancies begin with a normal cell quietly accumulating cancer-causing mutations and passing them on to its pre-cancerous children. This lesion can fester for years, but over time these mutations can twist the shapes and structures of healthy tissues into a jungle of deformities. Often once a tumor is found, it’s an array of warped cells, many with vastly different appearances and features, all cobbled together like a cursed mosaic.
The diversity of tumor cells is part of cancer’s threat. Some of those cells can — and often do — pick up distinct abilities like growing aggressively, spreading across the body, or resisting certain therapies. The technology inside Weissman’s mice helps to disentangle some of the details of that evolution by creating a molecular ancestry record in every cancer cell.
This works by using a protein called Cas9, which scientists use to engineer mutations into genetic material, and engineered rolls of DNA inside the mouse’s cells that serve as a molecular record book. The scientists engineered their mice to carry these components, and together they make a molecular machine. The protein progressively scribes mutations into this DNA record, which then get passed down to all the cell’s descendants. “The Cas9 is constantly online, randomly making marks at different locations in that sort of scratch pad,” Weissman said. “So, when two cells share the same mark in the same place, that’s because it happened in an ancestor.”
Once the expert researchers engineered these mice, they forced the mice to inhale a virus that activated the molecular record book as well as common cancer-causing mutations in the mouse’s lung cells. “Then you wait months and over time, a subset of them grow and form a mass,” Weissman said. “Some of those cells get additional changes and become cancerous, and we’re able to follow how they evolved.”
At the end of the study, the investigators took the tumors out of the mice and analyzed them one cell at a time, looking for two main things. First, they looked at which genes were turned on in each cancer cell. That gave the scientists an idea of physical traits the cell had and whether it bore any resemblance to other healthy cell types — like other lung cells, gastric cells, or cells from other tissues.
Photo by: SAUL LOEB/AFP/GETTY IMAGES
104 Marathons in 104 Days

Meet Jacky: 104 Marathons in 104 Days
Jacky Hunt-Broersma, 46, has run 26.2-miles every day since mid-January, normally taking around five hours. On Saturday, she completed her 104th consecutive marathon in as many days – an achievement she expects to be certified by Guinness World Records. A spokesperson said certifying the record would take around three months.
Waking up on Sunday – a day off at long last – was a bizarre experience for Jacky. “Part of me was really happy to be done,” she tells the BBC from her home in Arizona. “And the other part kept thinking I need to go running.” Her body is also recovering from the record-chasing effort, despite having stopped. “I feel tighter than I have the whole 104 marathons,” she admits. But Jacky – who was born and raised in South Africa, and has also lived in England and the Netherlands – is grateful. Because running has given her the confidence she was afraid she would never regain.
In 2002, doctors in the Netherlands diagnosed her with Ewing’s sarcoma, a rare type of bone cancer. Within two weeks, they amputated her left leg to save her life. She was only 26 years old. “It was a rollercoaster,” she recalls. “Everything happened so fast.”
For the first couple of years, Jacky struggled with the change in her life. She was angry that she had got cancer and embarrassed to be different. She wore long trousers in public so people would not notice the prosthetic. Almost on a whim, she took up running in 2016.
Jacky Decides on Marathon Goal
She had cheered her husband on at long-distance running events but had never considered doing it herself, thinking it was only “for crazy people”. Buying a special prosthetic for long-distance runners, she signed up for her very first 10K (6.2 mile) run. On the eve of the race, she switched her registration to the half-marathon category – and she has not looked back since, exploring longer distances and different terrains. “I’m an all or nothing person, so I just threw myself in,” she explains. “I love pushing boundaries and seeing how far I can push.”
At the beginning of the year, Jacky gave herself a new goal: the record for most consecutive marathons. The female Guinness record stood at 95 – set two years go by Alyssa Amos Clark, a non-amputee runner from Vermont – who did it as a pandemic coping strategy. The male Guinness record is held by Enzo Caporaso of Italy with 59 – although Spanish ultra-runner Ricardo Abad reportedly ran 607 consecutive marathons, finishing in 2012. So Jacky – a mother of two who works as an endurance coach – started running with the record in mind, making sure she always ran at least the length of a marathon.
She did the world-famous Boston Marathon in Massachusetts and the Lost Dutchman in Arizona, but marathons are not scheduled every day, so she also ran on local dirt paths, neighbourhood trails and even her own treadmill at home.
And when British runner Kate Jayden broke Alyssa’s record by completing 101 runs, Jacky kept going to beat her and “to round the month [of April] off” with one final marathon.
All told, she ran 2,734 miles. Guinness World Records told the AP news agency it would take around 12 to 15 weeks to review the evidence and certify the record.
Documenting those runs on social media, Jacky has raised over $88,000 (£70,000) for Amputee Blade Runners, a non-profit organisation that provides running blades like hers to amputees.
The runs have been mostly a mental game, she says, but they have also taken a physical toll.
Written by: BBC News
Photo Credit: Twitter account @NCrunnerjacky
Good News and Cautions about Pregnancy for Childhood Cancer Survivors

Some good news for childhood cancer survivors
First, the good news: Survivors of childhood cancer who became pregnant in adulthood are as likely to have healthy babies as those without a history of cancer, according to a new study. Their children also didn’t have higher risks of birth defects or other health problems at birth.
However, the study does suggest that these women face other pregnancy risks that may warrant more intensive obstetric care. For example, women who had been treated for cancer as children had higher risks of several severe complications during pregnancy, delivery, and the period after delivery.
The results were published January 19 in the Journal of the National Cancer Institute.
“The message here is largely positive,” said study leader Paul Nathan, M.D., of the Hospital for Sick Children in Toronto, Canada. “Women who have a history of childhood cancer have a really good chance of getting pregnant, and most of them are quite fine through the pregnancy. But it’s super important for the people caring for them to know about these risks.”
In the United States, many health care providers may not know if a patient was treated for cancer as a child, especially if they’ve moved between medical systems, cities, or states, explained Emily Tonorezos, M.D., director of NCI’s Office of Cancer Survivorship, who was not involved with the new study.
“High-risk obstetric care is widely available in most of the country, but childhood cancer survivors may not be recognized as needing that kind of care,” she said.
Beyond fertility, to pregnancy for childhood cancer survivors
Major progress has been made in treating many childhood cancers over the last several decades. Today, about 85% of children diagnosed with cancer will live for 5 or more years, compared with about 58% in the 1970s. Many of these cancers will never return.
These successes have allowed researchers to turn some of their focus to making treatments less toxic and improving the quality of life for survivors of childhood cancer as they grow up.
“When you talk with adolescents and young adults about their big post-cancer concerns, fertility is very high on that list,” said Dr. Nathan.
Cancer treatments can potentially affect future fertility for both women and men. For example, radiation therapy to or near the abdomen, pelvis, or spine can harm nearby reproductive organs. Radiation therapy to the brain can also damage the pituitary gland, which helps control the production of certain hormones needed for pregnancy.
Some types of chemotherapy can affect the ovaries, causing them to stop releasing eggs and estrogen. Having been treated for cancer during childhood can also affect sexual health, body image, and financial stability during childbearing years.
Many studies have focused on fertility preservation, with promising results. Women and girls now have several options that can help preserve their fertility, including freezing embryos or eggs. And new technology holds promise for boys undergoing cancer treatment before they’re old enough to freeze sperm.
Fewer studies to date have focused on what happens during pregnancy for survivors of childhood cancer. Despite the shortage of data, international guidelines were recently published to help doctors counsel their patients who are survivors about any specific pregnancy-related issues, explained Dr. Tonorezos.
The guidelines were an important first step, she continued.
“But more research to better understand the risks during pregnancy for childhood cancer survivors is urgently needed,” she said. “I think there are some lingering fears among survivors about pregnancy after cancer.”
Mostly safe, some risks for women
For their study, Dr. Nathan and his colleagues examined data captured by the single-payer health insurance program covering Ontario, Canada. They identified about 4,000 women who had been treated for cancer between 1985 and 2012 before the age of 21.
The team matched each of the 4,000 women to five other women who weren’t treated for cancer before age 21 by age and postal code, and then compared reported pregnancies between the two groups. They also compared the risks of miscarriage past 20 weeks into pregnancy, as well as the risks of more than 40 other health problems (for both mothers and children).
The researchers found that cancer survivors were just as likely to carry their pregnancy past 20 weeks. However, about 9% of babies born to survivors were preterm (defined as birth before week 37 of pregnancy), compared with around 6% of babies born to women who had not been treated for cancer.
There was no difference in birth defects or Apgar scores (a screening test used at birth to determine the baby’s need for additional medical services) between babies born to cancer survivors and the women in the control group.
Survivors didn’t have higher risks of preeclampsia, gestational diabetes, or caesarean delivery. However, they were at higher risk for several other complications, including heart problems and severe complications during or after birth. Several aspects of patients’ medical or treatment history were associated with specific pregnancy complications.
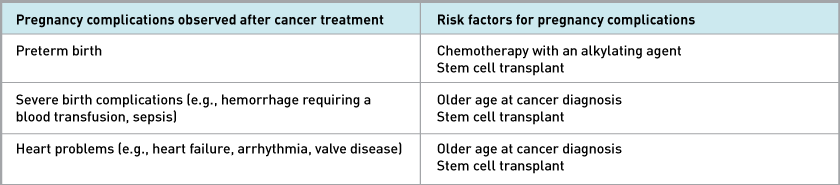
Overall, by age 30, the survivors were somewhat less likely than women not treated before the age of 21 to have been pregnant. About 22% of cancer survivors in the study had a recorded pregnancy, compared with about 27% of women not treated for a childhood cancer.
The databases used in the study did not collect information on whether women were unable to conceive. However, other studies have also shown fewer pregnancies among cancer survivors, wrote Hazel Nichols, Ph.D., of the University of North Carolina, and Daniel Green, M.D., of St. Jude Children’s Research Hospital, in an accompanying editorial.
Such trends indicate that “to fully support cancer survivors, it is also essential to consider the indirect consequences of an early cancer diagnosis, including disruptions to relationships, impacts on sexual health, and the potential for financial hardship, as additional challenges to parenting goals,” they wrote.
Childhood cancer survivors recognizing the need for high-risk obstetric care
Overall, the number of serious complications were fairly small. Only 87 out of more than 4,000 survivors (about 2%) experienced either a severe complication during labor or developed a heart problem during pregnancy. However, cancer survivors were twice as likely to experience either issue as women not treated for cancer.
And the potential impacts of these complications can be severe. Women who were treated for cancer before the age of 21 would benefit from discussions with their doctors about whether they need a referral for high-risk obstetric care, said Dr. Nathan. Such care can include monitoring a woman’s heart throughout pregnancy, as well as frequent fetal monitoring.
Most pregnant survivors are seen by family doctors or obstetricians who may know nothing about their cancer history or these specific risks, Dr. Nathan said. “[Figuring out] how to share this information with health care providers is going [to be] one of our key goals,” he added.
Health care providers’ knowledge of a patient’s cancer history can also spur other important conversations about reproductive health. For example, some women go through menopause early after taking certain chemotherapy drugs, Dr. Nathan said. That can shrink their window for conceiving—or pursuing fertility preservation techniques—compared with women who haven’t been treated for cancer.
“The burden of making sure you’re getting good health care is very often on the survivor and their family,” said Dr. Tonorezos. “That’s not where the burden should be, but survivors need to [make sure] health care providers have some of that information, because sharing data is not built into our health system,” she added.
Future research that would be helpful to survivors hoping to become pregnant could include testing which prenatal care strategies provide the most benefits in terms of preventing dangerous complications, Dr. Tonorezos said.
But overall, these results are encouraging, she said. “The expectation of a healthy pregnancy and a healthy baby should be the norm, even for childhood cancer survivors,” she said.
By: National Cancer Institute Cancer Currents Blog 3/4/22
Photo credit: iStock
Woman With Tumor as Heavy as Bowling Ball to Have ‘Very Complex Surgery’

A woman has set out to raise awareness of a rare form of cancer as she is due to have a 17.6-pound tumor removed from her body.
The 39-year-old U.K. woman, Stephanie Coles, was diagnosed with her condition in December after finding a lump on her abdomen, the BBC reported. A doctor initially thought that the lump may have been an enlarged spleen, but when Coles turned up at the hospital in pain shortly afterwards, they decided to investigate further.
A scan revealed leiomyosarcoma, or LMS, which is a type of soft tissue sarcoma that grows in smooth muscles. These muscles are in the hollow organs of the body, such as the intestines, stomach, bladder and blood vessels.
The condition is described by the U.S. National Cancer Institute as a rare, aggressive cancer that can grow quickly. According to one estimate, LMS accounts for between 7 and 11 percent of all soft tissue sarcomas and soft tissue sarcomas account for just 1 percent of all adult cancers in the U.S., the National Organization for Rare Disorders (NORD) states.
Is an LMS Tumor Genetic?
It isn’t known exactly what causes LMS to form, though some genetic conditions have been associated with it, including hereditary retinoblastoma and Li-Fraumeni syndrome, according to the National Cancer Institute.
Coles was told that cancer treatments like chemotherapy and radiotherapy wouldn’t work on her tumor and would cause damage to her internal organs. Instead, doctors will have to carry out a complex surgery to remove it.
[Photo credit:YAZGI BAYRAM/GETTY]
Atrium Health Levine Cancer Institute Awarded Highest Level of Achievement for Excellence in Person-Centered Care by Planetree Awards International

Levine Cancer Institute is the only cancer center in United States and one of two worldwide to earn this prestigious recognition
CHARLOTTE, N.C., Feb. 15, 2022 – Levine Cancer Institute (LCI) has once again been awarded Gold Certification for Excellence in Person-Centered Care by Planetree International. In 2017, LCI became the first cancer center in the world to earn the top designation for patient-centered cancer care delivery. Since then, LCI has diligently continued to expand their level of commitment to patients. LCI optimizes the patient experience with a focus on the active participation of patients and their families throughout the healthcare process, with an emphasis on partnership, compassion, transparency, inclusion, and quality. This unwavering dedication to patients has led to LCI’s latest recognition by the Planetree International Organization.
The Person-Centered Care Certification® acknowledges the organization’s achievement and innovation in the delivery of person-centered care, with the Gold Certification for Excellence in Person-Centered Care being the highest level of achievement based on evidence and standards. As documented by this international honor, LCI is dedicated to delivering world-class treatment that never overshadows its commitment to the real people, families and lives touched by the care provided by LCI teammates.
“The Planetree award helps us to focus each day on the needs and concerns of our patients and their caregivers,” said Derek Raghavan, MD, president of Atrium Health Levine Cancer Institute. “While we consistently focus on all the medical aspects of care, we don’t neglect the nuances and subtleties that are part of making patients feel safe and among friends. Our Planetree commitment extends to all aspects of our treatment and research and to all parts of our community.”
What is biomarker testing?
What is biomarker testing for cancer treatment?
Biomarker testing is a way to look for genes, proteins, and other substances (called biomarkers or tumor markers) that can provide information about cancer. Each person’s cancer has a unique pattern of biomarkers. Some biomarkers affect how certain cancer treatments work. Biomarker testing may help you and your doctor choose a cancer treatment for you.
There are also other kinds of biomarkers that can help doctors diagnose and monitor cancer during and after treatment. To learn more, visit the Tumor Markers fact sheet.
Biomarker testing is for people who have cancer. People with solid tumors and people with blood cancer can get biomarker testing.
Biomarker testing for cancer treatment may also be called:
- tumor testing
- tumor genetic testing
- genomic testing or genomic profiling
- molecular testing or molecular profiling
- somatic testing
- tumor subtyping
A biomarker test may be called a companion diagnostic test if it is paired with a specific treatment.
Biomarker testing is different from genetic testing that is used to find out if someone has inherited mutations that make them more likely to get cancer. Inherited mutations are those you are born with. They are passed on to you by your parents.
How are biomarker tests used to select cancer treatment?
Biomarker tests can help you and your doctor select a cancer treatment for you. Some cancer treatments, including targeted therapies and immunotherapies, may only work for people whose cancers have certain biomarkers.
For example, people with cancer that has certain genetic changes in the EGFR gene can get treatments that target those changes, called EGFR inhibitors. In this case, biomarker testing can find out whether someone’s cancer has an EGFR gene change that can be treated with an EGFR inhibitor.
Biomarker testing could also help you find a study of a new cancer treatment (a clinical trial) that you may be able to join. Some studies enroll people based on the biomarkers in their cancer, instead of where in the body the cancer started growing. These are sometimes called basket trials.
For some other clinical trials, biomarker testing is part of the study. For example, studies like NCI-MATCH and NCI-COG Pediatric MATCH are using biomarker tests to match people to treatments based on the genetic changes in their cancers.
To find out if there are open trials for which you may be eligible, use the search tool at Find Clinical Trial. Or, contact the Cancer Information Service for help.
Is biomarker testing part of precision medicine?
Yes, biomarker testing is an important part of precision medicine, also called personalized medicine. Precision medicine is an approach to medical care in which disease prevention, diagnosis, and treatment are tailored to the genes, proteins, and other substances in your body.
For cancer treatment, precision medicine means using biomarker and other tests to select treatments that are most likely to help you, while at the same time sparing you from getting treatments that are not likely to help.
The idea of precision medicine isn’t new, but recent advances in science and technology have helped speed up the pace of this area of research. Scientists now understand that cancer cells can have many different changes in genes, proteins, and other substances that make the cells grow and spread. They have also learned that even two people with the same type of cancer may not have the same changes in their cancer. Some of these changes affect how certain cancer treatments work.
Even though researchers are making progress every day, the precision medicine approach to cancer treatment is not yet part of routine care for most patients. But it’s important to note that even the “standard” approach to cancer treatment (selecting treatments based on the type of cancer you have, its size, and whether it has spread) is effective and is personalized to each patient.
Should I get biomarker testing to select cancer treatment?
Talk with your health care provider to discuss whether biomarker testing for cancer treatment should be part of your care. Doctors usually suggest genomic biomarker testing (also called genomic profiling) for people with cancer that has spread or come back after treatment (what’s called advanced cancer).
Biomarker testing is also done routinely to select treatment for people who are diagnosed with certain types of cancer—including non-small cell lung cancer, breast cancer, and colorectal cancer.
It’s also a good idea to check with your health insurance provider to see if they will cover biomarker testing for your cancer. Biomarker testing is not available at every hospital. Check with your health care provider to see if biomarker testing is offered at the hospital or place where you get your cancer care.
How is biomarker testing done?
If you and your health care providers decide to make biomarker testing part of your care, they will take a sample of your cancer cells. If you have a solid tumor, they may take a sample during surgery. If you aren’t having surgery, you may need to have a biopsy of your tumor.
If you have blood cancer or are getting a biomarker test known as a liquid biopsy, you will need to have a blood draw. You might get a liquid biopsy test if you can’t safely get a tumor biopsy, for example, because your tumor is hard to reach with a needle.
Your samples will be sent to a special lab where they will be tested for certain biomarkers. The lab will create a report that lists the biomarkers in your cancer cells and if there are any treatments that might work for you. Your health care team will discuss the results with you to decide on a treatment.
For some biomarker tests that analyze genes, you will also need to give a sample of your healthy cells. This is usually done by collecting your blood, saliva, or a small piece of your skin. These tests compare your cancer cells with your healthy cells to find genetic changes (called somatic mutations) that arose during your lifetime. Somatic mutations cause most cancers and can’t be passed on to family members.
Are there different types of biomarker tests?
Yes, there are many types of biomarker tests that can help select cancer treatment. Most biomarker tests used to select cancer treatment look for genetic markers. But some look for proteins or other kinds of markers.
Some tests check for a single biomarker. Others check for many biomarkers at the same time and may be called multigene tests or panel tests. One example is the Oncotype DX test, which looks at the activity of 21 different genes to predict whether chemotherapy is likely to work for someone with breast cancer.
Some tests are for people with a certain type of cancer, like melanoma. Other tests look for biomarkers that are found in many cancer types, and such tests can be used by people with different kinds of cancer.
Some tests, called whole-exome sequencing, look at all the genes in your cancer. Others, called whole-genome sequencing, look at all the DNA (both genes and outside of genes) in your cancer.
Still other biomarker tests look at the number of genetic changes in your cancer (what’s known as tumor mutational burden). This information can help figure out if a type of immunotherapy known as immune checkpoint inhibitors may work for you.
Biomarker tests known as liquid biopsies look in blood or other fluids for biomarkers from cancer cells. There are two liquid biopsy tests approved by the Food and Drug Administration (FDA), called Guardant360 CDx and FoundationOne Liquid CDx.
What do the results of a biomarker test mean?
The results of a biomarker test could show that your cancer has a certain biomarker that is targeted by a known therapy. That means that the therapy may work to treat your cancer. The matching therapy may be available as an FDA-approved treatment, an off-label treatment, or through participation in a clinical trial.
The results could also show that your cancer has a biomarker that may prevent a certain therapy from working. This information could spare you from getting a treatment that won’t help you.
In many cases, biomarker testing may find changes in your cancer that won’t help your doctor make treatment decisions. For example, genetic changes that are thought to be harmless (benign) or whose effects are not known (variant of unknown significance) are not used to make treatment decisions.
Based on your test results, your health care provider may recommend a treatment that is not FDA approved for your cancer type, but is approved for the treatment of a different type of cancer that has the same biomarker as your cancer. This means the treatment would be used off label, but it may work for you because your cancer has the biomarker that the treatment targets.
Some biomarker tests can find genetic changes that you may have been born with (inherited) that increase your risk of cancer or other diseases. These genetic changes are also called germline mutations. If such a change is found, you may need to get another genetic test to confirm whether you truly have an inherited mutation that increases cancer risk.
Finding out that you have an inherited mutation that increases cancer risk may affect you and your family. For that reason, your health care provider may recommend that you speak with a genetic healthcare provider (such as a genetic counselor, clinical geneticist, or a certified genetic nurse) to help you understand what the test results mean for you and your family.
Will biomarker testing for cancer treatment help me?
Biomarker tests don’t help everyone who gets them. There are several different reasons why they may not help you. Biomarker testing may not help you if:
- you are unable to safely get a biopsy needed for testing.
- there is not enough tumor tissue in your biopsy sample to have biomarker testing done.
- the test doesn’t find any biomarkers in your cancer that match with available therapies.
- the test identifies a matching therapy that would be used off label, and your insurance doesn’t cover the cost.
- the test identifies a matching therapy that is being tested in a clinical trial, and you are not able to participate in the trial.
Even if your test finds a biomarker that matches an available treatment, the therapy may not work for you. Sometimes other features of your cancer or your body affect how well a treatment works, such as how the medicine is broken down in your body.
Another reason the treatment might not work is that not all of your cancer cells have the same biomarkers. That means that a biomarker test may find a treatment that will kill some, but not all, of your cancer cells. Cancer cells that are not killed by the treatment could keep growing, preventing the treatment from working or causing the cancer to quickly come back.
One other reason biomarker tests might not help is because the biomarkers in your cancer can change over time. But a test only captures a “snapshot” of the changes at one point in time. So, the results of a biomarker test done in the past may not reflect the biomarkers in your cancer now. Your health care provider may want to test your cancer again, for example, if it comes back after treatment.
How much does biomarker testing for cancer treatment cost?
The cost of biomarker testing varies widely depending on the type of test you get, the type of cancer you have, and your insurance plan.
For people with advanced cancer, some biomarker tests are covered by Medicare and Medicaid. Private insurance providers often cover the cost of a biomarker test if there is enough proof that the test is required to guide treatment decisions. Tests without enough proof to support their value may be considered experimental and are likely not covered by insurance.
Many clinical trials involve biomarker testing. If you join one of these clinical trials, the cost of biomarker testing might be covered. The study coordinator can give you more information about related costs.
Originally published by the National Cancer Institute. Updated 12/14/21.
Photo credit: Caroline Davis 2010. CC BY 2.0
Can mRNA Vaccines Help Treat Cancer?
The coronavirus pandemic has thrown a spotlight on messenger RNA (mRNA)—the molecule that carries a cell’s instructions for making proteins. Hundreds of millions of people worldwide have received mRNA vaccines that provide powerful protection against severe COVID-19 caused by infection with SARS-CoV-2.
As stunningly successful as the mRNA COVID-19 vaccines have been, researchers have long hoped to use mRNA vaccines for a very different purpose—to treat cancer. mRNA-based cancer treatment vaccines have been tested in small trials for nearly a decade, with some promising early results.
In fact, scientists at both Pfizer-BioNTech and Moderna drew on their experience developing mRNA cancer vaccines to create their coronavirus vaccines. Now, some investigators believe the success of the mRNA COVID-19 vaccines could help accelerate clinical research on mRNA vaccines to treat cancer.
“There’s a lot of enthusiasm around mRNA right now,” said Patrick Ott, M.D., Ph.D., who directs the Center for Personal Cancer Vaccines at the Dana-Farber Cancer Institute. “The funding and resources that are flowing into mRNA vaccine research will help the cancer vaccine field.”
Dozens of clinical trials are testing mRNA treatment vaccines in people with various types of cancer, including pancreatic cancer, colorectal cancer, and melanoma. Some vaccines are being evaluated in combination with drugs that enhance the body’s immune response to tumors.
But no mRNA cancer vaccine has been approved by the US Food and Drug Administration for use either alone or with other cancer treatments.
“mRNA vaccine technology is extremely promising for infectious diseases and may lead to new kinds of vaccines,” said Elad Sharon, M.D., M.P.H., of NCI’s Division of Cancer Treatment and Diagnosis. “For other applications, such as the treatment of cancer, research on mRNA vaccines also appears promising, but these approaches have not yet proven themselves.”
With findings starting to emerge from ongoing clinical trials of mRNA cancer vaccines, researchers could soon learn more about the safety and effectiveness of these treatments, Dr. Sharon added.
How do mRNA vaccines work?
Over the past 30 years, researchers have learned how to engineer stable forms of mRNA and deliver these molecules to the body through vaccines. Once in the body, the mRNA instructs cells that take up the vaccine to produce proteins that may stimulate an immune response against these same proteins when they are present in intact viruses or tumor cells.
Among the cells likely to take up mRNA from a vaccine are dendritic cells, which are the sentinels of the immune system. After taking up and translating the mRNA, dendritic cells present the resulting proteins, or antigens, to immune cells such as T cells, starting the immune response.
“Dendritic cells act as teachers, educating T cells so that they can search for and kill cancer cells or virus-infected cells,” depending on the antigen, said Karine Breckpot, Ph.D., of the Vrije Universiteit Brussel in Belgium, who studies mRNA vaccines.
The mRNA included in the Pfizer-BioNTech and the Moderna coronavirus vaccines instructs cells to produce a version of the “spike” protein that studs the surface of SARS-CoV-2.
The immune system sees the spike protein presented by the dendritic cells as foreign and mobilizes some immune cells to produce antibodies and other immune cells to fight off the apparent infection. Having been exposed to the spike protein free of the virus, the immune system is now prepared, or primed, to react strongly to a subsequent infection with the actual SARS-CoV-2 virus.
Cancer research led to speedy development of mRNA vaccines
When the pandemic struck, mRNA vaccine technology had an unexpected opportunity to demonstrate its promise, said Norbert Pardi, Ph.D., of the University of Pennsylvania Perelman School of Medicine, whose research focuses on mRNA-based vaccines.
“The production of mRNA vaccines today is easy, fast, and can be scaled up as needed,” Dr. Pardi continued. The same manufacturing procedure can be applied to any mRNA sequence, he added.
Historically, the process of developing vaccines has taken 10 to 15 years. But both the Pfizer-BioNTech and the Moderna COVID-19 vaccines—the latter of which was developed in collaboration with NIH—were designed, manufactured, and shown to be safe and effective in people in less than a year.
“To develop an infectious disease vaccine during a pandemic, you need to be fast,” said Lena Kranz, Ph.D., co-director of Cancer Vaccines at BioNTech. “The current pandemic has confirmed our hypothesis that mRNA technology is well suited for fast vaccine development and rapid manufacturing on a global scale.”
The groundwork for the speedy design, manufacturing, and testing of the mRNA COVID-19 vaccines was established through decades of work on cancer vaccines. During this period, immunotherapy, including drugs such as immune checkpoint inhibitors, emerged as a new approach to treating cancer, leading, in some people, to dramatic and long-lasting responses.
“There’s a lot of synergy between research on immunotherapy and mRNA cancer vaccines,” said Robert Meehan, M.D., senior director of clinical development at Moderna. “Vaccines are building on the success of immune checkpoint inhibitors and expanding our knowledge of the underlying biology.”
Modifying and protecting the cargo of mRNA vaccines
Technologies that can deliver mRNA to the body are essential for the success of these vaccines. If an mRNA sequence were injected into the body without some form of protection, the sequence would be recognized by the immune system as a foreign substance and destroyed.
A solution employed by some investigational cancer vaccines is to encase the mRNA in lipid nanoparticles, which are tiny spheres that protect the mRNA molecules. Other delivery vehicles include liposomes, which are also a type of vesicle, or bubble.
“The most advanced mRNA-based vaccine platform uses mRNA encapsulated in lipid nanoparticles,” said Dr. Pardi. Now that the Pfizer-BioNTech and the Moderna coronavirus vaccine trials have demonstrated the effectiveness of lipid nanoparticles, the technology could certainly be used in future cancer vaccine trials, he added.
Another key feature of the Pfizer-BioNTech and the Moderna coronavirus vaccines is the use of modified forms of mRNA, according to Jordan Meier, Ph.D., of NCI’s Center for Cancer Research, who studies mRNA modifications.
The mRNA in these vaccines incorporates pseudouridine, which is a modification of a naturally occurring nucleoside. Nucleosides are the building blocks of mRNA, and the order of specific nucleosides determines the instructions that mRNA gives to the protein-making machinery in cells.
“The [pseudouridine] modification seems to make the mRNA itself almost invisible to the immune system,” said Dr. Meier. The modification does not alter the function of the mRNA but may enhance the effectiveness of the vaccines, he added.
Cancer researchers have been testing both modified and unmodified forms of mRNA in their investigational treatment vaccines. More research is needed to better understand the relative advantages of each approach for the development of cancer vaccines, Dr. Meier said.
Developing and testing personalized mRNA cancer vaccines
For more than a decade, cancer researchers have been developing a type of treatment known as a personalized cancer vaccine using various technologies, including mRNA and protein fragments, or peptides.
The investigational mRNA vaccines are manufactured for individuals based on the specific molecular features of their tumors. It takes 1 to 2 months to produce a personalized mRNA cancer vaccine after tissue samples have been collected from a patient.
“Speed is especially important for individualized cancer vaccination,” said Mathias Vormehr, Ph.D., codirector of Cancer Vaccines at BioNTech. “A highly individualized vaccine combination must be designed and produced within weeks of taking a tumor biopsy.”
With this approach, researchers try to elicit an immune response against abnormal proteins, or neoantigens, produced by cancer cells. Because these proteins are not found on normal cells, they are promising targets for vaccine-induced immune responses.
“Personalized cancer vaccines may teach the immune system how cancer cells are different from the rest of the body,” said Julie Bauman, M.D., deputy director of the University of Arizona Cancer Center.
Dr. Bauman is co-leading a clinical trial testing a personalized mRNA vaccine in combination with an immune checkpoint inhibitor in patients with advanced head and neck cancer. The study initially included patients with colorectal cancer, but this group did not appear to benefit from the therapy.
For patients with head and neck cancer, however, the early results were positive. Among the first 10 participants, 2 patients had all signs of their tumors disappear following treatment, known as a complete response, and another 5 had their tumors shrink.
“We were surprised to see two complete and enduring responses in our first group of patients with head and neck cancers,” said Dr. Bauman, noting that the study has been expanded to include 40 patients with the disease.
“The number of patients treated is small, but we are cautiously optimistic,” she added. The study is sponsored by Moderna, which makes each personalized vaccine in about 6 weeks.
The manufacturing process starts with the identification of genetic mutations in a patient’s tumor cells that could give rise to neoantigens. Computer algorithms then predict which neoantigens are most likely to bind to receptors on T cells and stimulate an immune response. The vaccine can include genetic sequences for up to 34 different neoantigens.
The promise of personalized immunotherapy with mRNA vaccines is “being able to activate T cells that will specifically recognize individual cancer cells based on their abnormal molecular features,” said Dr. Bauman.
Advancing the science of mRNA cancer vaccines
“A lot of immunotherapies stimulate the immune response in a nonspecific way—that is, not directly against the cancer,” said Dr. Ott. “Personalized cancer vaccines can direct the immune response to exactly where it needs to be.”
Some companies are also investigating mRNA cancer vaccines that are based on collections of a few dozen neoantigens that have been linked with certain types of cancer, including prostate cancer, gastrointestinal cancers, and melanoma.
In addition to clinical trials, fundamental research on mRNA cancer vaccines continues. Some investigators are trying to enhance the responses of immune cells to neoantigens in mRNA vaccines. One study, for example, aims to improve the responses of T cells that become exhausted while attacking tumors.
A challenge for the field is learning how best to identify neoantigens for personalized mRNA cancer vaccines, several researchers said.
“There’s still a lot we need to learn and many questions to answer,” Dr. Ott said. It’s not yet clear, for example, how personalized cancer vaccines should be best combined with other treatments, such as immune checkpoint inhibitors, he added.
As cancer researchers pursue these questions, other investigators will be developing knowledge from the growing number of people around the world who are receiving mRNA coronavirus vaccines.
Insights about the composition of mRNA or the way mRNA is packaged that emerge from studies of viruses could potentially inform work on cancer vaccines, said Dr. Breckpot.
“Unfortunately, it took a pandemic for there to be broad acceptance of mRNA vaccines among the scientific community,” she added. “But the global use of COVID-19 mRNA vaccines has demonstrated the safety of this approach and will open doors for cancer vaccines.”
“Can mRNA Vaccines Help Treat Cancer?” was originally published by the National Cancer Institute.
Photo credit: Discover Magazine
The Challenges of Living with Metastatic Cancer from Scan to Scan

Since 2018, Bethany Ross has started a new job, run four half marathons, and been treated for metastatic cancer.
The 33-year-old software engineer was diagnosed with stage IV neuroendocrine cancer 3 years ago, after vomiting every day for months. Doctors at the Dana-Farber Cancer Institute found tumors in her appendix and pancreas and cancer cells that had spread to her liver and nearby lymph nodes.
After two surgeries and hormone injections to treat her symptoms, Ross received good news: Doctors could no longer detect cancer in her body. She currently is not receiving any treatment for cancer, but every few months for the rest of her life, Ross will go to Dana-Farber for tests, including imaging scans, to see if the cancer has started to grow again.
“My doctors say the disease will come back at some point—they just can’t tell me when,” said Ross, who lives in New Hampshire. “With each scan, I wonder if this is the one that will reveal a recurrence.”
But Ross is not just waiting for the cancer to come back. She works full time and runs. She has also spoken at medical conferences, including a recent NCI-sponsored workshop, about her experience living with metastatic cancer.
Ross is part of a growing population of individuals who are living longer with advanced or metastatic cancer than was once possible.
“New treatments, such as targeted therapies and immunotherapies, have led to a real transition in survivorship,” said Jennifer Temel, M.D., of Massachusetts General Hospital, who studies cancer survivors and spoke at the NCI conference.
“People can stay on these treatments for many years, which means they can survive for many years,” Dr. Temel added.
Until recently, long-term survivors of advanced or metastatic cancer have primarily been women with metastatic breast cancer. But doctors are now seeing survivors with other types of cancer, including lung, gastrointestinal, kidney cancer, and melanoma.
The emergence of a growing population of people living with advanced or metastatic cancer has raised questions about the unique needs of these individuals and how to improve their care.
Igniting a New Field of Metastatic Cancer Research
To address these questions, NCI sponsored a virtual meeting that brought together researchers, health care providers, patient advocates, and people like Ross who are living with advanced or metastatic cancer.
The meeting featured presentations by survivorship researchers and people living with advanced or metastatic disease, as well as panel discussions. Each panel included at least one person living with cancer.
“We came together to exchange ideas about how we are caring for these patients and what we can do better,” said Temel. “Our goal is to ignite a new field of research to better support and address the care needs of patients with advanced cancers.”
People living with advanced or metastatic cancer have needs that may differ from those of people who have been treated for early-stage cancers, noted Lisa Gallicchio, Ph.D., of NCI’s Division of Cancer Control and Population Sciences (DCCPS), who co-led the meeting.
Examples of these needs include the management of chronic conditions, psychosocial support, caregiver support, financial support, and communication around the goals of care.
“People with advanced or metastatic cancer might require treatment for the disease indefinitely, or they might be on and off treatment for the rest of their lives,” Dr. Gallicchio said. “They will also likely undergo regular testing to identify signs of a recurrence.”
The Psychological Impact of Uncertainty
Although newer therapies can help some patients live longer, clinicians cannot predict how long a treatment is going to be effective for an individual patient. “The psychological impact of this uncertainty on patients and their loved ones was a theme of the [NCI] meeting,” said Dr. Temel.
Jamil Rivers, who was diagnosed with metastatic breast cancer 3 years ago at age 39, spoke at the conference about the uncertainty of living with the disease.
“When you learn that you have metastatic cancer and see the survival statistics, it can be overwhelming emotionally,” said Rivers. “And if you’re living with metastatic cancer, you’re living from treatment to treatment, from scan to scan.”
Rivers said that her latest imaging scans had not shown any tumors. “But I still have metastatic cancer,” she explained. “I have to be on some type of treatment to keep that cancer at bay so that it doesn’t grow and wreak havoc on my body.”
Rivers also described financial challenges related to cancer. She did not tell her employer about her diagnosis so that she could maintain her salary and her family’s health insurance, which was through the employer. She continued to work for the year that she received chemotherapy.
“Life doesn’t stop when you get diagnosed with cancer,” Rivers said in an interview after the meeting. “I have a family to take care of. We have a house, and I need to put food on the table and buy the kids clothes.”
Rivers has founded the Chrysalis Initiative, a nonprofit organization that aims to improve the lives of women of color with breast cancer, who have historically had poorer outcomes than other women with the disease. She has also shared her story through the national media, putting a spotlight on the needs of people living with metastatic cancer and their loved ones.
At the conference, Rivers issued a call to action: “For all future studies and initiatives around cancer survivorship, we should ask: How does this research also help meet the needs of patients with metastatic cancer?”
Helping Patients with “Scanxiety”
The stress that often accompanies the routine imaging scans that patients undergo to monitor changes in their health is sometimes called “scanxiety.”
“Scanxiety is a real phenomenon,” said Dr. Temel. “It’s natural to feel anxious when you’re waiting for an important test result, and I don’t think there’s a quick fix to it.”
Providing patients with information they can understand about their diagnosis and treatment is one way that Dr. Temel tries to support her patients and lessen their stress. “We know that when patients have accurate information, they are better prepared and make more appropriate decisions about the future,” she said.
She also conveys a message to her patients and families: “We’re going to be here for you whether the scan result is good news or bad news, and we have a plan for the future.”
This reassurance may make the period of anxiety and worry slightly less distressing, Dr. Temel said. Then she added, “I hate waiting for test results, too. It’s part of being human.”
Including Many Perspectives
Emily Tonorezos, M.D., director of NCI’s Office of Cancer Survivorship, said the conference created opportunities for researchers, clinicians, advocates, and people living with advanced cancer to exchange ideas. A publication summarizing the main discussions is in the works.
“The importance of including the perspectives of patients and survivors in designing, conducting, and interpreting research findings emerged as a theme of the meeting,” said Michelle Mollica, Ph.D., of the Healthcare Delivery Research Program in DCCPS, who co-led the meeting.
Christine Hodgdon, a patient advocate who is living with metastatic breast cancer and moderated a session at the meeting, said the presence of people living with advanced cancer on every panel conveyed an important message: Researchers need to hear from people who are living with advanced cancer.
“This was the first meeting I’m aware of that focused specifically on survivorship and advanced cancer,” added Hodgdon, who lives in Maryland and co-founded the organization Guiding Researchers and Advocates for Scientific Partnerships (GRASP), which brings researchers and patients together as equal partners.
“We believe there is a need to involve people with advanced disease in research and not just as participants in clinical trials,” said Hodgdon. Patients could help plan a trial, she suggested, or assist even earlier in the process, when researchers are asking, “What should I study?”
Following Long-Term Survivors over Time
Investigators at the meeting stressed the need for large longitudinal studies that follow people living with advanced or metastatic cancer over time, collecting information on the cancer types, treatments, and health histories of long-term survivors. Very few such studies exist, but they could help identify the unmet needs of patients and strategies for addressing these needs.
Data from longitudinal studies could also reveal clues about why some patients with metastatic cancer survive for extended periods and potentially how to help more patients live longer, several researchers said. But they cautioned that the research will be challenging.
Long-term survivors are “an incredibly heterogeneous” group, Dr. Gallicchio noted. “These individuals are from diverse backgrounds and have different cancer diagnoses,” she continued. “They have also been treated with different therapies or treatment regimens.”
Exactly how many people are living with advanced or metastatic cancer is not known, but a 2017 study found that the number of women living with metastatic breast cancer had been increasing.
Supporting Caregivers and Coordinating Care
At the conference, many participants stressed the need to learn more about how best to support the caregivers and family members of long-term survivors.
Rivers, who has three children, shared some challenges.
“Parents who are living with metastatic cancer may need help ensuring that their kids are supported emotionally,” she said after the meeting. “Cancer treatments have a lot of side effects, and it can be both scary and challenging to have conversations about these side effects with your family.”
Another challenge is coordinating care among various health care providers. People living with advanced or metastatic cancer often receive new treatments, and oncologists may need to communicate with primary care physicians about which side effects and possible complications to expect and how to address them.
Health care providers also have limited information about the long-term side effects of newer treatments, which is another reason that the coordination of care and communication among providers is important, several researchers noted during the NCI meeting.
As new treatments for cancer are developed and cancer care improves, the importance of understanding the needs of people living with metastatic or advanced cancer will increase.
“The science is advancing so rapidly,” said Bethany Ross. “With these new and highly effective therapies, more groups of patients are going to be living for longer periods of time.”
Clinical Trial Paper Published in Prestigious AACR Journal

The Clinical Trial
The Paula Takacs Foundation provided funding for the Phase II clinical trial of pembrolizumab in combination with doxorubicin in metastatic and unresectable soft tissue sarcoma at Levine Cancer Institute, enrolling 30 patients between 2017 and 2019. The paper was honorarily presented at American Society of Clinical Oncology’s Virtual Meeting in May 2020 and has recently been accepted for publication by the American Association for Cancer Research’s Clinical Cancer Research journal. The OnlineFirst version was published on September 2, 2021. Access the Abstract.
Why So Important?
We are incredibly proud to have provided funding for this clinical trial. This study gave pediatric and adult patients and families in the Charlotte region access to a new and novel treatment option, keeping 30 patients and families from traveling great distances for care. It gave so many families the hope they need. In fact, the Objective Response Rate of enrolled patients was almost 37%, which is extremely significant for soft tissue sarcoma trials. And, in fact, there were even some exceptional, long-term responders.
The results of the study were encouraging to researchers and could result in a larger, randomized Phase 3 study of this kind.
Through funding this clinical trial, the Paula Takacs Foundation enabled new, local treatments that could help patients. The publication of the paper expands global hope as researchers around the world learn from this study at Levine Cancer Institute in Charlotte, NC.
Seeing a Promising Future for Progress against Childhood Cancer

Childhood Cancer: Examples of Recent Progress
1982, Dr. Mariano Barbacid, a researcher working at NCI, and his colleagues identified a gene, called NTRK, that could transform healthy cells into cancer cells. Four years later, some of the same researchers reported that their initial discovery was only partially correct. The gene they had discovered refashioned healthy cells into cancerous cells only when it was joined to another gene, a molecular event known as a gene fusion.
Decades of further study defined how NTRK works under normal circumstances and how its improper activation causes cancer. These discoveries formed the basis for the development of drugs called NTRK inhibitors that were later shown to be highly effective against cancers that are fueled by gene fusions that involve NTRK. Given their impressive activity in clinical trials, NTRK inhibitors were recently approved by the FDA for the treatment of cancers with NTRK fusions, which occur in children and adults.
The success of NTRK inhibitors is not only a testament to the importance of basic science but also an excellent example of recent progress that’s been made for children with cancer. There are, I’m happy to say, many other examples.
Among the most well-known is the development of CAR T-cell therapies that can cure some children with very advanced forms of leukemia. Perhaps less familiar are the Children’s Oncology Group (COG)-led clinical trials that have pioneered ways of making often curative treatments for some children with cancer far safer, sparing kids from some short- and long-term treatment side effects, including hearing loss and infertility.
In recognition of Childhood Cancer Awareness Month, I want to reflect on the progress that’s been made against cancers that largely affect children.
For example, acute lymphoblastic leukemia (ALL) was uniformly lethal in children prior to the 1950s, but now, with modern approaches to this disease, more than 90% of children with ALL are cured. Overall, the mortality rate from all types of cancer among children and teens has dropped by more than 50% since 1980, and the substantial majority of kids with cancer today are cured of their disease.
But any discussion of progress also requires that we recognize where advancement has lagged. For some types of childhood cancer, such as soft tissue and central nervous system cancers, long-term survival is still poor and treatment advances have been limited. Moreover, children cured of their cancer may face a lifetime of health problems caused by their disease and its treatment, including aggressive surgeries, radiation, and chemotherapy.
These lingering disappointments have strengthened the resolve and commitment of the research community to discover innovative ways to cure as many children with cancer as possible—and to do so in a manner that causes the least long-term side effects for survivors. In my view, we are taking the necessary steps to achieve that end.
Data Leading the Way
I’m particularly excited about the radical transformation in the collection of data on children with cancer and the expanded ability to share it across the research community.
Data may not seem like the most compelling topic. But with efforts being conducted as part of the Childhood Cancer Data Initiative (CCDI), we are laying the groundwork for learning from every child with cancer. CCDI, I should note, builds on other NCI activities supported by the STAR Act, federal legislation enacted in 2018 to accelerate progress against childhood cancers.
I’ve met with researchers from across the country who specialize in pediatric cancer, and I can confirm that they are excited about this new world of data collection and sharing.
Take, for example, one CCDI-related program called the National Childhood Cancer Registry. This registry is collecting and linking data on diagnosis, outcomes, treatments, and long-term side effects for nearly every child with cancer in the United States.
Another CCDI effort, a national Molecular Characterization Protocol, will facilitate the collection of tumor tissue from children who have cancers for which such tissue for research is lacking or inadequate. A priority will be placed on cancers for which existing treatments are limited or ineffective.
As part of this protocol, researchers will perform in-depth molecular characterization (e.g., whole-genome sequencing and RNA sequencing) of this tumor tissue. Those data can be shared with patients’ oncologists to help enroll kids in precision medicine clinical trials and help guide their care and will also be available to pediatric cancer researchers through tools like the Genomic Data Commons.
Having access to such comprehensive molecular information that is linked to each patient’s clinical data (e.g., treatments received, stage of cancer) will provide unprecedented insights into the drivers of childhood cancers and how they become resistant to treatment, as well as factors that influence the risk of treatment-related side effects. It can also help identify potentially powerful combinations of targeted therapies, which I believe will be critical to improving outcomes.
These data and resources also will help provide answers to questions that can’t necessarily be addressed through clinical trials. Collecting comprehensive data from as many children as possible will give researchers a more thorough understanding of how well treatments work in “real world” populations. These data will also make it easier for researchers to monitor the health of survivors of childhood cancer throughout their lives, providing further insights into the impact of cancer and its treatments.
Advancing Precision Medicine in Childhood Cancer
A problem in clinical oncology is knowing the best treatment to give a patient. There are many medicines to treat cancer, and they can be combined with surgery and radiation in various complex regimens. But given all these possible choices for therapy, it is often not clear what is the best treatment for a given patient.
Currently, pediatric oncologists usually make treatment choices for their patients based on the best available evidence from historical clinical trials. For the child, and their family, this means starting therapy and waiting to see if those choices were effective.
For many children, that may mean going on treatment for a few months, and then having imaging scans done to see if the cancer is regressing. But it’s also a few months where the cancer might be getting worse, a few months of potential side effects, a few months of costs associated with treatment, and a few months of anxiety and distress for the child and their loved ones.
It would be far better to be able, at the time of diagnosis, to know which treatment approach is most likely to work. Determining the best treatment would rely not just on findings from previous trials but also specific information about the patient and their cancer. We don’t collect this molecular information uniformly today—and even when we do collect it, we don’t know how to interpret it completely to make these therapeutic decisions, particularly in children.
That’s where efforts like those being developed under CCDI come into play. And it’s also why precision medicine trials like the NCI–COG Pediatric MATCH trial (and its companion trial in adults, NCI-MATCH) are so important. Trials like Pediatric MATCH—and similar studies being conducted in EuropeExit Disclaimer and AustraliaExit Disclaimer—are teaching us how to use DNA, RNA, and protein data to identify the most effective treatments for each individual child’s cancer.
Although time will tell, I’m hopeful that these studies will help point the way to important answers about more effectively treating cancer, identifying new targeted therapies and treatment combinations that are highly effective in children.
Advancing Immunotherapy for Children with Cancer
Over the past decade, immunotherapy has offered a true paradigm shift in how we think about treating cancer. Although its impact has been greatest in adults, immunotherapy is also changing how we treat some children with cancer.
Several CAR T-cell therapies, for example, are approved to treat children and adolescents with leukemia and have led to cures for a modest proportion of children with very advanced disease.
NCI continues to be a leader in advancing CAR T-cell therapies for childhood cancer, leading early-phase clinical trials of new types of CAR T cells. We’ve also launched an initiative to manufacture CAR T-cell therapies to be used in clinical trials being run at multiple centers across the country. This initiative is already expanding the number of children who can participate in trials of CAR T-cell therapies and offers the hope of moving these new therapies into everyday patient care much more rapidly.
NCI also played a crucial part in advancing dinutuximab (Unituxin) to become a standard immune-based treatment for children with neuroblastoma. Dinutuximab’s molecular target, a protein on cancer cells called GD2, is also the target of a promising CAR T-cell therapy. NCI is supporting an early-phase trial of this GD2 CAR T-cell therapy for children with one of several types of solid tumor, including osteosarcoma, neuroblastoma, and melanoma. Another trial at Stanford University has already launched testing GD2 CAR T cells in children with a uniformly fatal form of brain cancer called DIPG.
And thanks to initiatives like the Cancer MoonshotSM-supported Pediatric Immunotherapy Discovery and Development Network, a path is quickly being blazed to expand immune-based treatments in children with cancer. That includes research to improve upon CAR T-cell therapies, support the development of other cellular therapies and other forms of immunotherapy, and expand their use to more types of childhood cancer.
The Imperative of Addressing Childhood Cancer Disparities
We should be encouraged by the progress that’s been made against childhood cancer, whether it’s improved survival outcomes using standard treatments like chemotherapy and radiation or novel therapies like bispecific antibodies.
But let me be clear: We must ensure that all children and adolescents with cancer will benefit equally from this progress.
Indeed, studies have documented disturbing racial/ethnic disparities in cancer incidence and survival rates. And, unfortunately, our youngest are not shielded from this harsh reality. Even for cancers that are highly curable, studies have found that Black and Hispanic children do worseExit Disclaimer than their White counterparts.
Numerous systemic and societal factors contribute to health disparities. That includes everything from underserved populations receiving less effective care, a lack of health care facilities in lower-income and rural areas, and the many problems that come with lower socioeconomic status, such as reduced educational attainment, increased exposure to environmental pollutants, and a higher likelihood of other health problems.
Given the structural and systemic nature of the causes of health disparities, directly resolving these societal problems is beyond the scope of a research agency like NCI.
Even so, NCI can and does support research that provides an evidence base for informing policy and clinical practice, advancing the science of disparities. Such studies include those that are allowing us to better understand the relative contribution of the factors that cause disparities, as well as those testing ways to help remedy disparities at the institutional and community level.
It also means supporting research to identify biological factors that contribute to disparities. For example, Hispanic/Latino children are not only at a higher risk than White children of being diagnosed with B-ALL, the most common form of leukemia, but even after accounting for factors like access to care and family income, these children have a higher risk of dying from the disease.
A recently published NCI-funded study identified a potential culprit that might contribute to this disparity: specific genetic changes, including a fusion gene, that are far more common in Hispanic/Latino children with B-ALLExit Disclaimer.
Why these changes are more common in Hispanic/Latino children with B-ALL is unclear, and so is exactly how they contribute to a worse prognosis. But these kinds of studies can identify children for whom standard treatments may not be sufficient and point the way to new, more effective treatment approaches for their specific cancers.
A More Hopeful Future for Kids
This is just a sampling of the research that I believe will, in coming years, expand the number of children with cancer who are cured, including those children with cancers that currently have few effective treatments.
Advances will come from many spaces, whether it’s the Cancer Moonshot-supported Fusion Oncoproteins in Childhood Cancer Consortium, studies of survivors of childhood cancer, or the many labs across the country working on new forms of cellular therapies.
And progress will come from basic science studies that, like the one Dr. Barbacid led all those years ago, were not specifically intended to address childhood cancer but, in the end, will save children’s lives.
, by Norman E. Sharpless, M.D., NCI Director
Photo Credit: National Cancer Institute/Jennifer Loukissas
2020 Impact Report

Our 2020 Impact Report is out!
Read how our supporters made it a chart-topping year in every way!
CLICK HERE to view, download and print the 2020 Impact Report.
Your support has been truly instrumental in developing this outstanding sarcoma research program, and I hope that you feel proud as you review this Impact Report. On behalf of myself and our Board of Directors, thank YOU for all you do to provide real HOPE for CURES.""From the many conversations I had with Paula Takacs, I know with all my heart that what we have achieved, and will continue to achieve, would make her leap with joy. With this first in-house clinical trial having been offered
to Levine Cancer Institute and Levine Children’s patients, our supporters have provided local access to cutting-edge treatments. Through testing a first-of-its-kind sarcoma blood biopsy technique developed at Levine Cancer Institute, patient treatment and disease monitoring may be revolutionized in the future. And as a result of other ongoing molecular research projects that are underway with your donations, there is hope of uncovering the drivers of various sarcomas so that future trials can be developed.
Susan Udelson
Executive Director
One Family’s Cancer Cluster: How He Uncloaked the Culprit
Family cancer clusters are frightening and not well-studied. Frankly, it takes courage (and dollars to cover expenses not often covered by insurance) to delve into the world of familial genetics. We don’t always like what we find. And honestly, many questions cannot yet be answered until researchers can bear fruit from the droves of genetic data that medical technology is able to lay at their fingertips.
Here’s one man’s emotional journey about how he decided to honor all of the family members he had lost to cancer, by uncloaking the painful genetic truths. I too embarked on genetic counseling, at Levine Cancer Institute, to see whether I could find out more about my cancer-ridden family tree, thinking that perhaps I could help my daughters have a greater change of lifelong health. Although today there is no specific genetic testing profile for sarcomas, the data that is now part of my permanent file can be re-analyzed at any time in the future as genetic knowledge and correlations progress.
Susan Udelson ~ Executive Director, The Paula Takacs Foundation
Cancer killed my mother, brother, and sisters. As the longest-living member of my family, I was determined to understand why
My Painful Lesson in Sarcoma Awareness
Honoring Alan through Sarcoma Awareness
In the very back of my file cabinet lies some seriously sacred territory – the many files documenting my brother’s medical history before sarcoma, records reflecting his fight against sarcoma, and his death certificate. I don’t know why I have kept these papers 7 years later, except to say that I thought they may help someone else needing research info, fighting an insurance appeal or filing for disability…or for assisting in the preventive care of Alan’s 3 children as they grow up. And then I must admit there was the emotional pain of shredding the papers that defined the most devastating chapter in my life, and deciding that it was easier on my heart to let them stay put.
I made the decision to pull out these files today in honor of Sarcoma Awareness Month, because I know in my heart that I do have an important story to tell you and a valuable lesson to impart. And what monumental thing did I learn after the loss of my brother, you ask? Awareness can potentially save your life, and the lack of it may kill you.
Like so many young people suddenly stricken with sarcoma, my brother Alan was a healthy young adult. However, his first “bolt out of the blue” health crisis came not from sarcoma, but from renal cell carcinoma in 2000. Alan had some unexplained and sudden back pain. He got it checked out quickly, and to his utter shock he had a malignant mass in his right kidney. Alan had his kidney immediately removed and had no further treatments, because there was no evidence of metastatic disease. Our family felt so grateful for this outcome and breathed a huge sigh of relief. But what we didn’t know at that time was that the ultimate enemy was waiting in the wings — and would strike without abandon.
Alan began to have regular oncologic visits and scans of his abdomen and pelvis after that 2000 diagnosis to monitor for reoccurrence or metastases of renal cell carcinoma. All was well with his cancer status…until it wasn’t at all. The new oncologist wrote this in his report 9 years later, in July 2009:
“I had the pleasure of meeting Mr. Stoller today for further recommendations regarding the role of adjuvant radiation therapy in the management of pleomorphic rhabdomyosarcoma of the right upper extremity, status post resection with evidence of biopsy-proven lung metastases. He is a charming 46-year-old gentleman who had a mass in the right upper extremity for approximately 10 years. This had been deemed to be a lipoma. However, after bringing this to the attention of one of his other physicians, the prompted an MRI on May 28, 2009. This revealed a 5.4×5.8x10cm inhomogeneous mass….”
What I will NEVER understand was why there were no physician notes about a significant lump on his bicep that was present THE ENTIRE 9 YEARS POST KIDNEY CANCER. Was anybody concerned about its mere presence in the backdrop of having had renal cell carcinoma? Were these oncologists familiar with sarcoma and what to look for? Was there such a complete lack of awareness on the part of every physician that saw my brother during that decade that no red flags were raised?
Sarcoma Awareness Grief
Let my brother’s tragic passing remind you to know your body, to question something that doesn’t seem right, to insist that your doctor take a thorough look, and to relentlessly be your own advocate. May it serve as a startling reminder that lumps, swelling, and pains need to be checked out thoroughly. And I mean THOROUGHLY. A two-second palpation of a lump on the arm of a cancer survivor doesn’t suffice as a lipoma diagnosis, in my humble opinion.
I will never know if Alan’s death would have been prevented if his physicians had been more thorough in their approach to his longstanding arm lump, or if he had insisted on a resection or biopsy 10 years prior to his sarcoma diagnosis. But what I can say with certainty was that the epicenter of this tragedy was a blatant lack of sarcoma awareness on everyone’s part. So I hope you’ll send this story to everyone you love with a mysterious lump, swelling or pain and implore them to take action. I hope you’ll share our foundation’s sarcoma awareness content on Facebook and Twitter not just during July’s Sarcoma Awareness Month, but throughout the year. It is my sincere prayer that we can work together towards a smarter tomorrow regarding sarcoma awareness. Many lives will depend on our diligent voices.
With love, light, and hope for more sarcoma awareness,
Susan
Our Joyful Sarcoma Stomp

By Sheila Mulcahy-Bell
The journey may be harsh, but in the end I pray many are able to stomp out sarcoma.
I knew nothing about sarcoma until an acquaintance of mine told me she had it and is now cancer free. When people think about cancer they think of the more “popular” cancers. Sometimes I think cancer gets swept under the rug when it comes to discussing the less “popular” ones and sarcoma in my eyes is one of them. I am joyful for the experience my family has had in learning about sarcoma through our participation in the 2017 Sarcoma Stomp, and in helping to try to raise awareness and money to find cures.
When we found out about the Sarcoma Stomp 5K, I knew I wanted to participate. What I didn’t know was that 5 out of 6 in my family would join in! (The 6th was there in thought, but a 5K isn’t her thing.) It was a delight to be able to join Julia’s Jamboree team to STOMP out sarcoma. Something I didn’t expect was that this event would also lead to our family agreeing they all wanted to do more 5K’s to raise awareness and money for more organizations. Most may think that this is no big deal, unless you have the “couch potato” thing going on in your family like we do. So I am proud and joyful about this new commitment!
Sometimes in life we get too busy — and forget to stop and think about what others are going through and how much they need prayers and a cure. I look at Julia and I am grateful for her strength and courage to have fought and beaten sarcoma. It has been an eye opener for me to remember to appreciate any time I have with family and friends, and the Sarcoma Stomp was just one more way I was able to spend time with them.
I am glad I was able to support the cause to help find cures for sarcoma. I look forward to the next Sarcoma Stomp event and hope that in the near future there will be cures.
Sheila
Rockin’ Wendie and Rainbow Wigs

I’ve wondered for a number of years now who Rockin’ Wendie was and I always admired Team Rockin’ Wendie’s Warriors at the annual Sarcoma Stomp. Tonight I finally found out in an email from Wendie’s sister and it felt SO good. Why? Because she didn’t just explain why this team shows up at the Stomp each year donning rainbow wigs, smiling brightly, and lighting up the course with their smiles. Heather told me the story of a woman so beloved, not only by her family and friends, but also by thousands of elementary school students learning the value of character traits through her music and dance.
“We are looking forward to coming to the Sarcoma Stomp once again this year,” says Wendie’s sister Heather Mitsopoulos. “We will be there with our wigs in tow! I don’t know if I’ve ever mentioned why we dress up the way we do, but my sister who had Sarcoma, Wendie, used to film these character trait videos that would get played in local elementary schools in Macon, GA where she lived. She played a character called Rockin Wendie and her co-star was Poppin Pj (a close family friend who wore a mohawk during the videos). Chick Fil-a was working on a contract with my sister to use the videos in their marketing materials, but unfortunately my sister got too sick to continue filming. The elementary age kids that the videos went to never knew she was sick or didn’t have any hair because she wore her wig. 🙂 So, we honor her memory by dressing up as Rockin Wendie and Poppin PJ! She joined us for 1 of the Sarcoma Stomps a few years ago and got to speak with Paula…shortly after that Sarcoma Stomp both Paula and my sister passed away. The Sarcoma Stomp falls usually within a few days of my sister’s b-day, so it’s a celebration of her b-day for us!”
Thank you for writing about your awesome sister, Heather! There is no doubt that the stories behind the mission gives this foundation texture and soul. And Wendie sure did have soul! :-)))
Click this link to watch a Rockin’ Wendie and Poppin PJ video: https://www.youtube.com/watch?v=f120n1K2CfU
Click to see a news story about Rockin’ Wendie and Poppin PJ: https://youtu.be/hOHL-C5eKe0
If you’d like to join the Rockin’ Wendie’s Warriors team, either in-person or as a Virtual Stomper, click HERE.
If you’d like to donate to the Rockin’ Wendie’s Warriors team, click HERE.



Defining “Cured” from the Sarcoma Trenches

It didn’t take me long after being diagnosed with sarcoma to come to the conclusion that cancer terminology can be really confusing. But here’s how I choose to see it…
How People Talk About “Cured”
Most folks gather with their friends at the local coffee joint to have light conversation, but when I see my fellow cancer survivors we might discuss things like the terms “cancer-free”, “in remission”, and “cured”. Through our conversations, it was apparent that the survivor, the oncologist, friends and family use the terms differently and at different times. Doctors treating sarcoma patients tend to celebrate NED (no evidence of disease), sight the statistics, and say that a patient is “in remission” because sarcoma cancer does often come back. Friends and family might say that once a removal surgery takes place or chemotherapy is finished that the cancer is gone, and feel that it is gone forever. But as one of those patients I debate in my own head about when a sarcoma patient is considered “cured”, because that’s the elusive term in sarcoma we’d all covet to use. I have tended to stay somewhere in the middle thus far in my journey — I know the cancer can return, but I focus on the positive. So in that middle space, should I tell everyone I am “cancer-free”? How do all these terms feel to those of us who have been diagnosed, whether in or out of treatment? How does that play into our emotional state and stress levels?
According to scientific data and terminology, I am in complete remission because no new cancer has been detected since its removal in October, 2015. Am I “cancer-free”? And when am I “cured”? CT scans cannot detect small cells. And I know that statistically, my sarcoma -if it is going to return- will most likely come back in 2-3 years. But from what starting point? Is it 2-3 years from the surgery, when it was removed, or is it 2-3 years from when I ended treatment (in my case, chemotherapy), about 6 months after the surgery and clear scan? Confused yet? I know many of us are.
After all, my oncologist gave me the option of doing one round of treatments (six cycles, each lasting 21 days). I could have opted out. But I asked myself–what if there were loose cancer cells floating around in my body that the scan had missed? How could I be sure I was truly “cancer-free” without a little chemo? Should I less confidently say I am “in remission” and then wait and see?
My View of “Cured”
Now I visit the radiologist every six months for a scan to see if any cancer large enough to see has returned. I anxiously await the call from my doctor saying that everything looks good. I know I will feel much relief when I can theoretically ring the bell and announce that I am FIVE years clear. Five years in the world of cancer generally means you are “cured”, though there are never any guarantees – especially with sarcoma.
Until then, I take one day at a time and look forward to the future as “chunks” of time. I will say I am doing well — I exercise, plan family activities and attempt not to think about it. I try not to focus on how I define my cancer state, or dwell in the anxiety that walks next to me 24/7 in the reality of these terms and statistics. Every day that I wake up and believe that I am “cancer-free” is a day I am very thankful.
Please join me in celebrating sarcoma survivorship, however you personally define it, by registering for the Sarcoma Stomp!!! Register for my team, Julia’s Jamboree, whether participating in-person or as a Virtual Stomper.
With love and hope,
Julia
By guest blogger and sarcoma survivor, Julia Greer
No Rare Disease Pity Party Here!

My family and friends will tell you that I’m a data dork, learn-a-holic and question queen. I guess that is a compliment? 😉 Since taking the helm at the foundation, I’ve been doing a lot of thinking about whether raising funds for a rare disease is more difficult than a mainstream one. I find it mysterious that total private philanthropy for sarcoma is paltry in the US. Why is that? What’s the downfall of our disease space, and how can we do markedly better? Aren’t there enough donors out there who care about sarcoma sufferers?
Trust me and keep reading, because 30 seconds from now you’ll agree that we can feel encouraged by the whopping success of another rare disease’s playbook…
Sarcoma’s public relations hurdle #1: What the heck is it?
It is a common nonprofit mantra that the key to raising funds for any cause is rooted in awareness. But what the heck does that truly mean? How does teaching the name of a disease name translate into donations down the line? Does imparting basic facts and statistics move people to open their hearts and their wallets? And, is fundraising success tied to disease incidence?
Just my opinion, but from my vantage point I think sarcoma may have a significant PR problem. Most people have never heard of it, have no clue what parts of the body it strikes, or understand how often it takes lives. Try finding a decent “What is sarcoma?” YouTube video. Maybe 3 in the world? Search Twitter for “#sarcoma” and see how many there are posts with that hashtag. Good luck. You can count on one hand most days.
Sarcoma is diagnosed only about 15,000 times per year. Do you find people have heard of it? Do you think the awareness issue is magnified due to the name of this cancer? After all, sarcoma is not named after a single body part, like breast, lung, colon, prostate, or pancreas. Its name does not give a hint that it is indeed a cancer, nor does the word help anyone visualize a body strike zone.
So have you heard of CF? Know what it is? I made a donation last year to the Cystic Fibrosis Foundation because my friend was fundraising for this cause. I knew that CF was a progressive, deadly genetic disease that causes persistent lung infections and limits the ability to breathe over time. And so, I opted to donate. In other words, I had heard of it and had some basic understanding of it. That certainly weighed into my decision to give the gift towards funding research, without having substantial knowledge of CF or knowing anyone suffering from CF.
I decided to look further out of curiosity, and was stunned to learn that CF is diagnosed only 1,000 times per year in the U.S.! And, only 30,000 are living with CF at any given time. (Under 200,000 diagnoses per year is considered a rare disease.) How did I come to be familiar with the name of this exceedingly rare disease? How did I have any knowledge about it? I have no idea!! Did my familiarity, as weak as it was, impact my desire to donate? Yes, absolutely!
Cause awareness – meaning familiarity of name and a basic definition – really matters in the world of fundraising.
Sarcoma public relations hurdle #2: Not enough awareness events means not enough public exposure
There are only a handful of organizations in the entire country devoted to sarcoma awareness and research, and only a short list of fundraising events. The national sarcoma organization is expanding from 5 walks to 9 this year (plus a few galas and patient education conferences), and was only formed in the year 2000. It is young!
Now look for cystic fibrosis organizations and you get tons, including the main CF Foundation, formed in 1955. So how big is CF Foundation given that the disease strikes only 1,000 times per year? The Foundation’s chapters hosted more than 1,000 events from coast to coast in 2015, netting $91 million. This includes more than 125,000 Great Strides walkers gathering in nearly 500 locations across the United and raising nearly $42 million. Mind officially blown.
I know that CF Foundation has a much longer history, but how has a disease that has an incidence of only 1,000 persons per year become so widely known and supported?? The very abbreviated answer is that they funded research extensively and eventually began their own affiliate to develop and test drugs. Some of these drugs became FDA approved and have extended life considerably for CF sufferers. It is truly an AMAZING nonprofit story which we can all learn from.
So, bottom line?
I think that this huge awareness deficit for sarcoma in the U.S. is costly in terms our collective ability to privately fund research, advance science, and ultimately improve survival rates. So how can we make a difference here in Charlotte, NC over the next few decades? Quite frankly, we’ve got to work hard, dream big and raise our voices. Can we continue to spread the word and become the largest run/walk for sarcoma in the US? Should we take the Sarcoma Stomp to other cities? Can our foundation one day raise millions per year and become one of the largest private funders of sarcoma clinical trials and research in this country? Can we become the gold standard? Can we become the role model?
Yes we can.
I want to read this blog post at my retirement gathering (lol) many years from now and hear the crowd audibly cheer as we celebrate our reach, our many milestones and the many curative treatments for sarcomas we have funded. Until then, we should not hide behind a rare disease pity party as a reason for not being able to raise substantial monies for research funding. Victim mentality always backfires. Let’s be more like Cystic Fibrosis in the decades to come. Think big, act big, be big!
So, tap the keys NOW to register for the April 29 Sarcoma Stomp, and let’s get that non pity party started… www.sarcomastomp.org
Life Awaits!

I get emotional – but in a good way – every time I meet someone in our sarcoma community and hear about their life. It’s a huge honor to meet a cancer survivor and hear their story, because I never forget that it is a very painful topic that invokes every emotion under the sun. I feel like I am treading on sacred ground in these moments. And that’s where I treaded last week.
Excitedly, I walked into the coffee shop to meet Sarcoma Stomp participant, Leah Kirby, for the first time. I was greeted by a tall, beautiful, glowing young woman. “How could she have been diagnosed with that devil?” was my first thought as I laid my eyes upon her. But my head told me that I knew better than to dwell in that mystery, since the horrid fact is that 40% of bone sarcoma sufferers are under age 35.
Leah told me that she was diagnosed with osteosarcoma on her right fibula at age 31. It all started with leg swelling, but she didn’t think much of it since she is a nurse practitioner at CMC Pineville — putting in many steps each day. A lump then appeared, but still no pain. That lump on her leg was watched for 4 or 6 months, as she remained pain-free but perplexed. Doctors decided to do an MRI in April of 2015, at which time the osteosarcoma was found. Leah had 2 cycles of chemotherapy before surgery and 4 cycles afterwards. Dr. Joshua Patt of Levine Cancer Institute removed a 11 ½ x 6 cm tumor from her leg, along with some muscle and nerves, miraculously achieving negative margins. For that surgical outcome, and for the fact that the disease had not metastasized to her lungs, Leah was so grateful.
Leah then paused our conversation and pulled out her phone, showing me – without any hesitation – a photo of that swollen leg. It sure didn’t look like the devil had taken up camp in there. But then I saw the photo of her extracted tumor; it was ghastly. It made my heart hurt.
“What things about being a young adult diagnosed with a sarcoma did you want your peers to understand?” I asked her. Here is what she told me:
- Please listen to your body! I had swelling and a lump in my leg, but no pain. As an NP on my feet all day, it didn’t seem very troubling at first. But then it was. No pain does not mean no problem exists. Pay attention people!
- Some people don’t understand that a cancer diagnosis is a marathon and not a sprint. They don’t understand “NED” (no evidence of disease), thinking that it means cancer-free. They ask me how long I must wait until I’m considered cured. The statistical fact is that I have a 45% chance of surviving 5 years. I just choose not to dwell on it or make it the epicenter of my world.
- Cancer is a life-changing diagnosis. For me it meant several huge decisions, like whether to delay starting chemotherapy to harvest some of my eggs or begin immediately and risk infertility. I tried so hard to stay true to myself to cope with 9 months of treatment. But it is hard because everything changes.
She went through these difficult topics with grace, candor, and wisdom way beyond her years. It was very clear that Leah had refused to let her osteosarcoma diagnosis define who she is or what life holds for her. In fact, she told me that she will be moving back to her home state of Illinois to be with her family and her boyfriend…and to write the next pages of her life’s story. She will travel before starting her new job. She is very happy. And it showed.
Leah let me know that she won’t be able to participate in the Sarcoma Stomp this year, since she’ll already be back in IL then. She is hoping, however, that some of her Charlotte buddies will continue to participate in honor of their friendship — and to raise money for sarcoma research at Levine Cancer Institute.
As we finished up and said our goodbyes, Leah took me over by the exit to meet her sweet mother. “Well, life awaits!” she exclaimed with eyes sparkling, as she took her mother’s hand, looked back at me, and strode confidently out the door.
Our Supporters Don’t Need the Nickel!

Supporters, What Do You Think?
During a recent trip to my mailbox, I retrieved a donation solicitation that yielded a familiar sight; one that I must admit, kinda irritates me. In the window of the envelope, near the familiar stream of return address labels, a shiny new nickel is on display for the taking. What kind of message is this sending to us? That 5 cents can change a person’s life? Or is it subliminally reinforcing what I see as a concerning and rising industry trend that we will give you a gift if you donate to our cause?
Okay, I’ve said it. Before you go all postal on me, please, hear me out.
It has been a little over two years since I took the helm of the Paula Takacs Foundation for Sarcoma Research. My background in the stock market and securities regulation is apples-and-oranges compared to the non-profit world, and boy have I learned a lot in the last 26 months. I’ve met many peers and have attended many events. I’ve watched, I’ve analyzed, and I’ve ingested a ton. To say that I am in awe of the endless stream of critical missions and passionate nonprofit leaders in a challenging landscape is an understatement. But inherent in the industry competition and the changing demographics of the donating public comes what I believe to be an unfortunate rising trend – the increased expenses of fundraising events related to giving party swag, participation gifts, and the like. Yes, sometimes these things are donated by corporate sponsors, but oftentimes they are absorbed by the nonprofits themselves. And that lessens the impact they can make.
So why are our supporters different? Why do they “get it”?
For every fundraiser we execute, whether it is the annual signature Sarcoma Stomp, or other smaller events held throughout the year, our Board pours over the numbers and makes conscious decisions about where we will allocate our expense budget to attract participants to our event and to ensure that the event is fun, engaging, and of quality. We make the tough choice not to give gifts for showing up, because we firmly believe that those who understand the huge significance of this mission will attend — and because they want to fund as much new research as possible. Are we taking a competitive risk? Yes. Can we sleep at night? Yes, because we feel most authentic and correct in this approach.
I have gotten to know many of our supporters, some of whom hail from sarcoma families and some who are just plain kind. Perhaps I’m a bit partial, but I think that we have the most loyal and heart-forward supporters around. Each year they donate, participate, and volunteer with vigor. They tell us that they had a blast at our events, and they send soulful emails and notes of gratitude for the work that we do. They get it. They feel connected to the cause, the effort we put forth, and the immense value of the sarcoma research program at Levine Cancer Institute.
So what is our philosophy of supporter connectivity and appreciation?
I would like to think that our connectivity lies in several factors, but all of them take root in authenticity and communication. We love getting to know our families – the stories of how they came to know us, the stories of how cancer has impacted their own life, the journeys of survival against the odds, and the heartbreaking retelling of loss. It is that candor and openness between us that is beautifully real. It is the complexity and the struggle of the human health experience in the cancer world that binds us in this mission.
Our supporters also understand how they directly impact the mission and how their generosity is put to work. They read the updates we send in emails and post to our website, they stay in touch on Facebook and Twitter, and they call me to ask questions. They truly believe that the research they are funding at Levine Cancer Institute is important, valuable, and novel. They are keenly aware that efforts to advance the field of cancer research requires significant funding and long-term commitment. They give generously even though they see that the impact on our community and the world-at-large is a lengthy process. They are committed. They get it.
We thank our supporters for their generosity, their embrace, and their understanding of us. Thank you for not making us feel badly that we don’t send you nickels in the mail to entice donations and that we don’t give you expensive swag for showing up at fundraisers. Instead, we show our gratitude in smiles, hugs, handwritten notes, and phone calls. We show our gratitude in the telling of the progress of the growing research program at Levine Cancer Institute. As things continue to advance at Levine, we believe you’ll be hearing from patients who’s lives have been improved by your tireless dedication. These are not expenses you’ll see on our balance sheet. This is how we choose to do business.
We look forward to a wonderful time with you all at the Sarcoma Stomp. They’ll be lots of smiles, hugs, and expressions of gratitude for all. Come introduce yourself if you are new to the Foundation family. Come ask questions about the progress. Yes, these things will be in our budget under “intangibles.” Nope, they’ll be no nickels in view.
What Is This Sarcoma Survivor Thankful For?

The holiday season brings a heightened awareness of gratitude, perspective, and introspection for all, but perhaps for cancer survivors even more so. Listen to Julia, a sarcoma survivor, as she tells us what she is grateful for.
Why Levine Cancer Institute?

It is important for our donors to know why our foundation has chosen to invest their gifts in sarcoma research at Levine Cancer Institute. Learn from Executive Director Susan Udelson why we made this choice, and how you can stay on top of all research project developments at the Institute.
Portraits in Courage: Fuzzy on a Mission

Tucked inside the One Wells Fargo Center in uptown Charlotte, you’ll find our next featured “Portrait of Courage”. She’ll be perched with a smile behind the register — and firmly in command — at the Omnibus Gift Shop. Her name is Kelly LaFlash — known to her family and friends as “Fuzzy”. She works hard each week managing all aspects of this cards and sundries outfit and serving her long-time customer base. And while she does that job really well, she is also on an important mission each day that’s very close to her heart.
When I sat down with Fuzzy it was instantly clear that she was on a mission. She wore a childhood cancer awareness sweatshirt adorned with gold ribbon pins and cancer buttons. Her wrists were covered in silicone bracelets sporting messages of hope and healing. There was no mistaking her billboard of passion for childhood cancer awareness. Why so visual, you ask?
Courage At Such a Young Age
Fuzzy was diagnosed with metastatic Rhabdomyosarcoma at the tender age of 14, after some persistent nosebleeds, coughing, and colds. She also had a lump on the side of her neck. It was during a related tonsil and adenoid surgery that the surgeon discovered a tumor in her nasopharynx. An intense chemotherapy and radiation treatment schedule followed, which led her family to give her the nickname “Fuzzy” (like the nursery rhyme Fuzzy Wuzzy) as her long locks fell out.
It is truly miraculous and joyful knowing that Fuzzy is with us today as a 34-year survivor. WOW! And with that incredible statistic through courage comes some important life lessons that she’d like to share with all of us.
Childhood cancer research receives very little funding, so all of us can do our part to make a critical difference. I know firsthand that every penny does count! Fuzzy maintains a donation jar on her checkout counter at Omnibus, and her loyal customer base throws in a bit of change here and there for whatever the current fundraiser is (She raises money at any given time for sarcoma and other pediatric cancer research through CureSearch, the Jeff Gordon Children’s Foundation, Still Brave Cancer Foundation, St. Baldrick’s Foundation, Isabella Santos Foundation, Claire’s Army, Kick-it for Kids’ Cancer, Cookies for Kids’ Cancer, and the Paula Takacs Foundation). These random money tosses into her jar have resulted in approximately $6,000 in donations to these nonprofits over the last 5 years! Simply remarkable!

- As a childhood cancer survivor, I’ve learned along the way to try to conquer my fears and to never lose my sense of humor! Fuzzy admits that anxiety and fear can easily become your steady sidekick – as fallouts from being a long-time survivor. She tells me she is much more confident many decades later and is most proud of pushing herself to learn how to drive, take to the dance floor, and ride in a helicopter in her thirties. She also reminds kids to find joy in their sense of humor throughout their cancer journey. “Most people have one of those days. I have one of those lives,” she says with a wink, but then quickly adds this quote: “Life isn’t about waiting for the storm to pass, it’s about learning to dance in the rain.” — Vivian Greene
- The most significant life lesson I can convey is that I choose to live this life of mine with a positive attitude. This quotes says it perfectly, and it has literally changed my life: “The longer I live, the more I realize the impact of attitude on life. Attitude, to me, is more important than facts. It is more important than the past, than education, than money, than circumstances, than failures, than successes, than what other people think or say or do. It is more important than appearance, giftedness or skill. It will make or break a company…a church…a home.The remarkable thing is we have a choice every day regarding the attitude we will embrace for that day. We cannot change our past…we cannot change the fact that people will act in a certain way…we cannot change the inevitable.The only thing we can do is to play on the one string we have, and that is our attitude.I am convinced that life is 10% what happens to me and 90% how I react to it. And so it is with you; we are in charge of our attitudes.” — Chuck Swindoll
So I hope you’ll drop by the Omnibus Gift Shop and see Fuzzy one of these days. She personifies ‘courage.’ Drop a coin in the jar, give her a hug, and tell her that she is an amazing Portrait of Courage.
Portraits in Courage: Dr. Corrie Painter

What do you get when you combine a brilliant biomedical scientist, a sarcoma diagnosis, and a mother load of courage? Answer: Dr. Corrie Painter, The Angiosarcoma Project, and our inaugural Portraits in Courage post.
I am in awe of her story, and you will be too. Although it starts as a life with a wonderful husband and two very young girls, turned upside down by a devastating cancer diagnosis, trust me when I say that this journey takes those lemons and squeezes out an astonishing truckload lemonade.
Corrie was diagnosed with primary breast angiosarcoma in May 2010 – at only 36 years old. This rare sarcoma (Nothing like being diagnosed with a RARE form of a RARE cancer. Gosh, I’ve learned to hate that word.) is diagnosed only 300 times per year globally, which strikes in the lining of the blood vessels of the body. It took numerous biopsies over a 5-month period to nail down a precise diagnosis and form a treatment plan – which Corrie sadly points out is way faster than normal for most angiosarcoma patients. She credits her surgeon at Dana Farber for making the call to perform a more radical surgery that “saved her life” since initially she was given months to live.
So how did Corrie learn about her disease and find support for this rare cancer? Being a scientist, Dr. Painter instinctively turned to PubMed, but these academic publications devastated her as she read the depressing bits of data. She also did Internet searches to try to find others with the diagnosis. When she did find names of people who were reaching out for connection and contacted them, she rarely got a response. That’s because she would find their obituary. Corrie said that each time “it was a black hole that opened up next to her and sucked out every ray of hope.”
In a last ditch attempt to learn and connect, she turned to Facebook and found the Angiosarcoma Cancer Group – formed by Lauren Ryan – with 10 people in it. Although a tiny group, they seemed to house the world’s knowledge of this disease. They knew which doctors to see. They knew side effects. Most importantly, they were all ALIVE! “We were instantly bound by something far greater than you can experience with another person outside of the bond of marriage and parent/child relationships,” says Corrie. (See https://www.facebook.com/groups/101899709845272/)
Lauren Ryan had also formed the Angiosarcoma Awareness Foundation, and together these tightly bound friends continued to nurture the nonprofit and the Facebook support group together. Corrie took the advocacy baton from the hand of her beloved friend in 2014 when she sadly passed away, and has continued the work on behalf of Lauren and all other sufferers. Today there are over 2,000 people in the Angiosarcoma Group on Facebook, and 100-200 at any one time actively exchanging information and supporting each other.
But Dr. Corrie Painter did not not stop there…not by a long shot…
Taking Courage a Giant Step Forward
Corrie realized that there was a potential treasure trove of data inherent in the interactions through Facebook. She was determined to find a way to look at these cases and begin generating data as to the underlying how’s and why’s of this cancer. She completed her PhD, then a fellowship in cancer immunology, and decided to pursue a career focused on patient advocacy and science.
And, now? Today, Dr. Painter is a grateful angiosarcoma survivor of 6 years (in remission!). She is the Associate Director of Operations and Scientific Outreach for the Metastatic Breast Cancer Project at the Broad Institute of MIT/Harvard. Starting in October of 2015, patients with Stage 4 metastatic breast cancer began authorizing the collection of tissue, saliva samples, and medical records for cataloging, study, and genomic testing. Already more than 2,000 patients from 50 states have stepped forward to advance research through this social media driven approach (see www.mbcproject.org for more information)! This project has been very well received by patients, who feel “first in class” in bringing translational medicine directly to them for the first time. Why? They feel connected to the entire process. They were engaged in things like website build out and the patient questionnaire. They send back personal notes and saliva kits that their children color directly to scientists – making everyone feel personally connected to each other and galvanized to the project. It has far exceeded everyone’s hopes and expectations. This same approach will be launched on September 1st for angiosarcoma, and Dr. Painter and the sarcoma community couldn’t be any more excited!!
The Broad hopes to take this same direct-to-patients initiative and apply it to this rare cancer that couldn’t otherwise be studied thoroughly. She is hoping to get 50-100 people living with the disease to go through the whole process of getting clinical information, tumor samples, saliva and perhaps blood. She wants to engage everyone still alive (or those family members who lost loved ones) to collect information in perpetuity in order to gain a clinical and genomic understanding of angiosarcoma. And our bet is on her! (See https://www.facebook.com/groups/1556795987968214/ to read the direct input by patients, families, and advocates to the Broad scientists as this Angiosarcoma Project continues to develop.)
As a scientist and as a patient, Dr. Painter believes that we need to have models where everyone at the table is learning from each other – patients, pharmaceutical companies, payers, doctors, and designers – and converging all of this into a better research system. Her vision at the Broad Institute is based upon a “learning health system”, where information isn’t lost, where patient experiences don’t happen in vein, and where we can all learn from each other because data isn’t silo’d off. Ultimately, resulting in better health outcomes. In fact, only a few weeks ago Corrie was personally invited by Joe Biden’s office to attend a Summit of the recently announced Cancer Moonshot initiative. As part of the big data working groups, she gave significant input about including research in the continuum of healthcare, including patient visit data being available for use in future clinical trials and other translational research in our country. “The healthcare system needs to become a learning system and not just a reactionary system,” says Dr. Painter.
All of us at the Paula Takacs Foundation honor Dr. Painter’s courage – not only to battle for the sake of her own health – but to bravely take center stage in the advancing of cancer research for thousands of other sufferers. We proudly stand behind her efforts, so stay tuned for updates on the Angiosarcoma Project later this year.
So is that some awe-inspiring lemonade, or what?
2021 Update: Since our story published, Dr. Painter launched numerous other patient-researcher direct collaboration studies, including the Metastatic Prostate Cancer Project, the Brain Tumor Project, the Osteosarcoma Project, and the Esophageal & Stomach Cancer Project. Corrie formed the nonprofit Count Me In, a consortium of the Emerson Collective, the Broad Institute and Dana-Farber Cancer Institute established to advance patient partnership research, responsible for advancing these studies.
Exercise: From Foe to Friend

Thank you to Ashley Smith of AWS Fitness for this passionate and heartfelt post!
Why exercise? Plain and simple….because you can!
With the Sarcoma Stomp 5K just weeks away, this is the perfect opportunity to examine why starting a fitness program is a necessity. As a personal trainer, I know that there are so many people out there that just DO NOT respond favorably to exercise. Meaning….there is nothing that they dread doing more. But, I am here to tell you that exercise must be an essential part of your life. If you are physically able, you have NO EXCUSE. If you aren’t exercising for YOU, do it for those who love you.
Instead of talking about all of the reasons that exercise is good for you (I think we all learned that in grade school Physical Education…nothing much has changed, folks), let’s talk about what inactivity does to our already AGING bodies. If you choose a sedentary lifestyle you are at risk for DIABETES, CARDIOVASCULAR DISEASE, JOINT AND LIGAMENT PROBLEMS, and OBESITY. And, remember how I mentioned AGING??? Well, to put it bluntly, a decline in how our brains and bodies function and perform starts at age 40. 40?!?! How do we slow that trend down? EXERCISE! It’s very simple.
I know that starting a program is hard and maybe you are telling yourself that you have tried it 20 times before. Maybe you stuck with it for a while and then quit. Maybe you failed all together and never even got past day one. Well, MAKE TODAY DIFFERENT by doing these three things for me.
- Choose a plan that will stick. Set realistic goals for yourself and don’t expect instant results. Change takes time. If you choose a plan that delivers gradual results and not one that breaks you down right out of the gates, you are more likely to stick with it. Find a couple of things that you really enjoy doing and do them….OFTEN….4–5 times/week.
- Get your friends and family on board with you. Exercise is much more fun if you have a friend that wants to work hard too. If you can’t find someone, sign up for some classes. More importantly, schedule them and PUT THEM ON YOUR CALENDAR. You are less likely to bail on things if they are actually scheduled in your day, week after week.
- Make a public commitment. We live in a public world these days. Like it or not, people know a lot about you. Why should this be any different? If you let others know that you are starting an exercise program, it will force you to have others hold you accountable. Set goals for yourself….maybe it’s losing weight, maybe its gaining strength, maybe it’s running a 5K (I happen to know one coming up in 3 weeks). Whatever it is, tell your friends about it and let them help you!
Finally, if you can take anything away from what I’ve said here, please let it be this. Your body requires a certain amount of love and respect to thrive. If you live your life saying, “I can’t do this” or “I’ll fail” or “It’s just too hard”, that mindset becomes who you are. Don’t let this negativity become your life experience. How do you know that this time won’t be the one time that it sticks? How do you know that you won’t start to love how you feel every single day?
Do it for yourself. Do it for your children. Do it for those that can’t. Do it because you can.
For Paula, and all Our Forever Friends, This Valentine’s Day

Gentlemen, do these scenes ring a bell?
The phone rings as you sit down to eat, and your girlfriend runs out of the house like a three-alarm fire is ablaze. Maybe you open your front door and spy your wife being handed a dozen roses by another woman. Or, your daughter tells you that she would rather go to the mall with her friends in tow then go car shopping for a hot-looking convertible.
I’m sure you often scratch your head in wonderment at the thinking process of the opposite sex. And I don’t blame you one bit. Women are complex and mysterious creatures! But fear not, for I believe these words will give you much insight into a very special part of our innate compasses. Quite simply, our girlfriends matter. And the older and wiser we become, the more entrenched we get in these soulful and beautiful relationships. A week without meaningful contact with a friend? Well, that’s like having the oxygen sucked out of our lungs.
After a half-century-plus living on this earth, I can say that I’ve been blessed with so many incredible friendships. I treasure each and every one, and have always considered them to be life-long relationships. But I never, ever thought about how to define what “life-long relationships” are until I began losing some friends to the “Big C”, cancer.
So now, I must redefine friendships and find a way to embrace my forever friends who have gone beyond the physical realm. Although there have been copious tears released as I think of my friends being farther away, I can tell you that my heart feels so much comfort in making the choice to believe that they still exist somewhere. I know they’re watching over us, and doing what only girlfriends can do for our souls.
Paula Takacs is one of my forever friends, living among the stars and watching over me. I am thinking about her today because the most tender of days, Valentine’s Day, will be her 42nd birthday! So, indulge me as I celebrate her and reminisce:
Paula, I remember your last birthday on earth, your 40th, when you were showered with countless expressions of love from every person you’ve blessed with your love. I remember you telling me how completely full your heart was and I remember you saying, “THIS WAS THE BEST BIRTHDAY I’VE HAD….EVER, EVER, EVER!”, despite your knowing that your health was failing rapidly. I remember looking at your frail body and hearing those words, and wishing that every single friend of ours could have been standing there with us. It was one of those take-your-breath-away moments…part of my “highlight reel” that reminds me yet again that to love and be loved is what we are ultimately striving for.
For your birthday, Paula, I’m doing a few things to honor you and make you smile. First, I launched a beautiful new website for your foundation! And guess what? I couldn’t have done it without another friend of mine, Camine Pappas, who poured her heart out in time, talent and love on this project. Another friendship honoring our forever friendship…how cool is that?
But that’s not all! We’ve opened registration for your beloved Sarcoma Stomp! I’m sure your forever friends will register in force like they always have, running their personal best or walking with their funky costumes. I’ve gotten to know some of these ladies over the last few years, and all I’ve got to say is that you sure do know how to pick ‘em! They are amazing women!
So here’s to you, Paula Takacs, my forever friend. I’m celebrating your birthday by asking every woman out there to think of a friend or a forever friend they’d like to spend some time with, or to honor, or to remember…and rejoice with them at the 2016 Sarcoma Stomp. It might be face-to-face or it might be in their hearts. But I have no doubt that, in doing so, they will feel the love of a forever friendship.
With love and friendship, today and always,
Sue
